
Hoe stamcellen ons helpen in de strijd tegen kanker
De voorbije jaren hebben wetenschappers een enorme vooruitgang geboekt in de strijd tegen kanker. Naast het gebruik van chemotherapie en radiotherapie (‘stralen’) kunnen ook onze eigen lichaamscellen aangewend worden om kankercellen te bestrijden. Zo spelen stamcellen een belangrijke rol in de behandeling van lymfeklierkanker. Hoe dat precies in elkaar zit, lees je in dit artikel.
Lymfeklierkanker
Het immuunsysteem zorgt voor de aanmaak van lymfocyten. Dat zijn cellen die ons helpen bij de afweer tegen vreemde indringers, bijvoorbeeld een virus. Sommige doen het rechtstreeks zelf (T-lymfocyten), andere maken antistoffen aan (B-lymfocyten). Deze cellen liggen verspreid over ons hele lichaam in het lymfeklierstelsel (oa in lymfeklieren en milt). Lymfeklierkanker ontstaat wanneer een van deze immuuncellen beslist autonoom te groeien. Een normale cel groeit volgens een bepaalde cyclus met ingebouwde controlepunten om de celgroei binnen de opgelegde grenzen te houden. Een tumorcel ontsnapt aan deze controlemechanismen en blijft ongeremd groeien. Vele cellen samen vormen een tumormassa. Op een gegeven moment is de tumormassa zo groot geworden dat we merken dat een persoon kanker heeft. We kunnen de vergrote lymfeklieren vol tumorcellen of een vergrote milt voelen of de zieke persoon vermagert omdat de tumorcellen al zijn energie opslorpen. Met deze klachten gaan zieke mensen naar de dokter. Deze stelt de diagnose door een stukje van zo’n lymfeklier weg te nemen (een lymfeklierbiopsie) en microscopisch te onderzoeken. De tumorcellen zien er onder de microscoop helemaal anders uit dan gewone cellen. De diagnose kanker wordt gesteld.
Autologe stamceltransplantatie
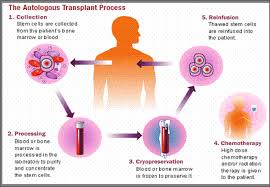
Stamcellen zijn cellen die kunnen uitgroeien tot eender welke cel in ons lichaam. Bij de geboorte beschikken we over heel wat stamcellen die delen en uitgroeien tot specifieke cellen met een bepaalde taak. Dergelijke cellen noemen we gedifferentieerde cellen. Er blijft echter ook een kleine voorraad stamcellen achter in een volwassen lichaam. Zo beschikken wij nu nog over cellen die eender welke cel in ons lichaam kunnen vervangen. Net zoals hart, long en nier getransplanteerd kunnen worden van een overleden donor naar een ontvanger, kunnen ook stamcellen getransplanteerd worden. Die stamcellen kunnen ofwel van de patiënt zelf afkomstig zijn (een autologe stamceltransplantatie) ofwel van een al dan niet verwante donor (een allogene stamceltransplantatie). De behandeling van kanker is erop gericht snel delende kankercellen uit te roeien. Dat doen we klassiek door het gebruik van chemotherapie of ioniserende stralen (radiotherapie). Helaas zijn er naast de tumorcellen ook heel wat gezonde cellen die door de chemotherapie en radiotherapie getroffen worden, zogenaamde ‘onschuldige slachtoffers’. Het gaat dan voornamelijk om cellen die snel delen, bijvoorbeeld de haarcellen (daarom verliezen sommige patiënten die chemotherapie krijgen hun haar) of de cellen in ons beenmerg. In ons beenmerg worden continu drie soorten cellen gemaakt: rode bloedcellen, witte bloedcellen en bloedplaatjes. De rode bloedcellen zorgen voor het transport van zuurstof doorheen het lichaam. De witte bloedcellen zorgen voor de afweer tegen infecties. De taak van bloedplaatjes is het vormen van klonters. Zo lopen we na een chemotherapiekuur een verhoogd risico op infecties, bloedingen en tekort aan zuurstofdragers. Wanneer we er echter in slagen om voor het toedienen van hoge dosissen chemotherapie stamcellen uit te zuiveren, hebben we minder schrik van het verlies van deze gezonde cellen. Dat is het principe van een autologe stamceltransplantatie (zie figuur 1). Daarbij krijgt de patiënt eerst een klassieke chemotherapiekuur. Voor het toedienen van hoge dosissen chemotherapie worden stamcellen door het geven van een groeifactor losgeweekt uit het beenmerg en gemobiliseerd in de bloedbaan. Via een bloedafname worden de stamcellen uit het lichaam gehaald en op zeer koude temperatuur bewaard. Vervolgens krijgt de patiënt hoge dosissen chemotherapie. We hopen dat de chemotherapie de tumorcellen overwint, helaas zullen onze gezonde snel delende cellen hierdoor ook in mankracht verliezen. Op een gegeven moment heeft de patiënt nog een bedreigend laag aantal rode bloedcellen, witte bloedcellen en bloedplaatjes over. Dan worden de stamcellen ontdooid en teruggegeven aan de patiënt. Deze stamcellen groeien dan weer uit tot rode bloedcellen, witte bloedcellen en bloedplaatjes en zorgen ervoor dat de patiënt minder risico heeft te overlijden ten gevolge van een levensgevaarlijke infectie of bloeding. Helaas is deze procedure niet zonder risico’s. Ondanks de enorme vooruitgang in dit soort behandeling de voorbije jaren overleeft ongeveer 3% een autologe stamceltransplantatie niet.
Resultaten bij patiënten met mantelcellymfoom
In mijn onderzoek ben ik gaan kijken naar de resultaten van autologe stamceltransplantatie bij patiënten met een mantelcellymfoom. Dat is een agressieve vorm van lymfeklierkanker waarbij B-lymfocyten ongeremd beginnen groeien. De 58 onderzochte patiënten kregen meteen na diagnose chemotherapie gevolgd door een autologe stamceltransplantatie. Uit de resultaten blijkt dat patiënten in complete remissie voor de transplantatie (alle tumorcellen uitgeroeid na de chemotherapie) minder snel hervielen dan patiënten in partiële remissie voor de transplantatie (nog een beperkt aantal tumorcellen aanwezig na de chemotherapie). Daarnaast heb ik vastgesteld dat de MIPI score (Mantle Cell Lymphoma International Prognostic Index) als scoresysteem in staat is de patiënten in te delen in verschillende prognostische categorieën met een verschillende totale overleving. Gezien 3% overlijdt ten gevolge van de stamceltransplantatie blijft de uitdaging voor de toekomst goed te selecteren welke patiënten voor een autologe stamceltransplantatie in aanmerking komen. Dat kan aan de hand van prognostische factoren, bijvoorbeeld de MIPI score en de hoeveelheid achtergebleven tumorcellen na de klassieke chemotherapie. Het is immers belangrijk om de tumor tot op de laatste cel uit te roeien voor de transplantatie. De ontwikkeling van nieuwe chemotherapeutische agentia speelt daarbij een belangrijke rol. Voorbeelden daarvan zijn antistoffen gericht tegen tumorspecifieke eiwitten. Mantelcellymfoomcellen exprimeren het eiwit CD20 op hun oppervlak met als gevolg dat deze tumorcellen aangevallen worden door de antistof “rituximab” specifiek gericht tegen CD20. Gezonde cellen die geen CD20 op hun oppervlak exprimeren, worden zo niet getroffen.
Besluit
Ondanks enorme vooruitgang is de strijd tegen kanker helaas nog niet gestreden. Bij het mantelcellymfoom steekt de kanker vroeg of laat weer de kop op. We zijn nog niet in staat een patiënt met een mantelcellymfoom definitief te genezen. Onderzoek blijft nodig om behandelingen te ontwikkelen die de tumor overwinnen, vooraleer de tumor ons overwint.
Bibliografie
1. Rule S. Frontline therapy and role of high-dose consolidation in mantle cell lymphoma. Hematology.
2016;419–24.
2. Dreyling M, Ferrero S. The Role Of Targeted Treatment In Mantle Cell Lymphoma: Is Transplant Dead
or Alive? Haematologica. 2016;101:104-114.
3. Vandenberghe E, Ruiz de Elvira C, Loberiza FR, Conde E, Lopez-Guillermo A, Gisselbrecht C, et al.
Outcome of autologous transplantation for mantle cell lymphoma: a study by the European Blood and
Bone Marrow Transplant and Autologous Blood and Marrow Transplant Registries. Br J Haematol.
2003;120:793–800.
4. Sweetenham JW. Stem cell transplantation for mantle cell lymphoma: should it ever be used outside
clinical trials? Bone Marrow Transplant. 2001;28:813–20.
5. Jantunen E, Canals C, Attal M, Thomson K, Milpied N, Buzyn A, et al. Autologous stem-cell
transplantation in patients with mantle cell lymphoma beyond 65 years of age: a study from the
European Group for Blood and Marrow Transplantation (EBMT ). Ann Oncol. 2012;23:166–71.
6. Khouri IF, Saliba RM, Okoroji G, Acholonu SA, Champlin RE. Long-Term Follow-Up of Autologous
Stem Cell Transplantation in Patients with Diffuse Mantle Cell Lymphoma in First Disease Remission:
The Prognostic Value of β 2 -Microglobulin and the Tumor Score. Cancer. 2003;98:2630–5.
7. Ganti AK, Bierman PJ, Lynch JC, Bociek RG, Vose JM, Armitage JO. Hematopoietic stem cell
transplantation in mantle cell lymphoma. Ann Oncol. 2005;16:618–24.
8. Kasamon YL, Jones RJ, Diehl LF, Nayer H, Borowitz MJ, Garrett-mayer E, et al. Outcomes of
Autologous and Allogeneic Blood or Marrow Transplantation for Mantle Cell Lymphoma. Biol Blood
Marrow Transplant. 2005;11:39–46.
9. Geisler CH, Kolstad A, Laurell A, Jerkeman M, Räty R, Andersen NS, et al. Nordic MCL2 trial update:
six-year follow-up after intensive immunochemotherapy for untreated mantle cell lymphoma followed
by BEAM or BEAC + autologous stem-cell support : still very long survival but late relapses do occur.
Br J Haematol. 2012;158:355-62.
10. Mangel J, Leitch HA, Connors JM, Buckstein R, Imrie K, Spaner D, et al. Intensive chemotherapy and
autologous stem-cell transplantation plus rituximab is superior to conventional chemotherapy for newly
diagnosed advanced stage mantle-cell lymphoma : a matched pair analysis. Ann Oncol. 2004;15:283–
90.
11. Vose JM, Bierman PJ, Weisenburger DD, Lynch JC, Bociek G, Chan WC, et al. Autologous
Hematopoietic Stem Cell Transplantation for Mantle Cell Lymphoma. Biol Blood Marrow Transplant.
2000;6:640-5.
12. Chaudhary L, Kharfan-Dabaja MA, Hari P, Hamadani M. Is hematopoietic cell transplantation still a
valid option for mantle cell lymphoma in first remission in the chemoimmunotherapy-era? Bone
Marrow Transplant. 2013;48:1489–96.
13. Alwasaidi TA, Hamadah A, Altouri S, Tay J, McDiarmid S, Faught C, et al. Outcomes of both
abbreviated hyper-CVAD induction followed by autologous hematopoietic cell transplantation and
conventional chemotherapy for mantle cell lymphoma: a 10-year single-centre experience with
literature review. Cancer Med. 2015;4:1817–27.
14. Damon LE, Johnson JL, Niedzwiecki D, Cheson BD, Hurd DD, Bartlett NL, et al.
Immunochemotherapy and Autologous Stem-Cell Transplantation for Untreated Patients With Mantle-
Cell Lymphoma : CALGB 59909. J Clin Oncol. 2009;27:6101–8.
15. Murali S, Winton E, Waller EK, Heffner LT, Lonial S, Flowers C, et al. Long-term progression-free
survival after early autologous transplantation for mantle-cell lymphoma. Bone Marrow Transplant.
2008;42:529–34.
16. Dreyling M, Lenz G, Hoster E, Vah Hoof A, Gisselbrecht C, Schmits R, et al. Early consolidation by
myeloablative radiochemotherapy followed by autologous stem cell transplantation in first remission
significantly prolongs progression-free survival in mantle-cell lymphoma : results of a prospective
randomized trial of the European MCL Network. Blood. 2005;105:2677–90.
17. Till BG, Gooley TA, Crawford N, Gopal AK, Maloney DG, Petersdorf SH, et al. Effect of remission
status and induction chemotherapy regimen on outcome of autologous stem cell transplantation for
mantle cell lymphoma. Leukemia & Lymphoma. 2008;49:1062-73.
18. Garcia-Noblejas A, Cannata-Ortiz J, Conde E, Gonzalez Barca E, Guttierrez N, Rojas R, et al.
Autologous stem cell transplantation (ASCT) in patients with mantle cell lymphoma: a retrospective
study of the Spanish lymphoma group (GELTAMO). Ann Hematol. 2017;96:1323–30.
19. Hermine O, Hoster E, Walewski J, Bosly A, Stilgenbauer S, Thieblemont C, et al. Addition of highdose
cytarabine to immunochemotherapy before autologous stem-cell transplantation in patients aged
65 years or younger with mantle cell lymphoma ( MCL Younger ): a randomised, open-label, phase 3
trial of the European Mantle Cell Lymphoma Network. Lancet. 2016;388:565–75.
20. Delarue R, Haioun C, Ribrag V, Brice P, Delmer A, Tilly H, et al. CHOP and DHAP plus rituximab
followed by autologous stem cell transplantation in mantle cell lymphoma : a phase 2 study from the
Groupe d’Etude des Lymphomes de l’Adulte. Blood. 2013;121:48–54.
21. Geisler CH, Kolstad A, Laurell A, Andersen NS, Pedersen LB, Jerkeman M, et al. Long-term
progression-free survival of mantle cell lymphoma after intensive front-line immunochemotherapy with
in vivo – purged stem cell rescue : a nonrandomized phase 2 multicenter study by the Nordic
Lymphoma Group. Blood. 2008;112:2687–94.
22. Andersen NS, Pedersen L, Elonen E, Johnson A, Kolstad A, Franssila A. Primary treatment with
autologous stem cell transplantation in mantle cell lymphoma : outcome related to remission
pretransplant. Eur J Haematol. 2003;71:73–80.
23. Widmer F, Balabanov S, Soldini D, Samaras P, Gerber B, Manz MG, et al. R-hyper-CVAD versus RCHOP/
cytarabine with high-dose therapy and autologous haematopoietic stem cell support in fit
patients with mantle cell lymphoma : 20 years of single-center experience. Ann Hematol. 2018;97:277–
87.
24. Romaguera JE, Fayad L, Rodriguez MA, Broglio KR, Hagemeister FB, Pro B, et al. High Rate of
Durable Remissions After Treatment of Newly Diagnosed Aggressive Mantle-Cell Lymphoma With
Rituximab Plus Hyper-CVAD Alternating With Rituximab Plus High-Dose Methotrexate and
Cytarabine. J Clin Oncol. 2005;23:7013–23.
25. LaCasce AS, Vandergrift JL, Rodriguez MA, Abel GA, Crosby AL, Czuczman MS, et al. Comparative
outcome of initial therapy for younger patients with mantle cell lymphoma: an analysis from the NCCN
NHL Database. Blood. 2012;119:2093–99.
26. Chihara D, Cheah CY, Westin JR, Fayad LE, Rodriguez MA, Hagemeister FB, et al. Rituximab plus
hyper-CVAD alternating with MTX/Ara-C in patients with newly diagnosed mantle cell lymphoma: 15
year follow up of a phase II study from MD Anderson Cancer Center. Br J Haematol. 2016;172:80–8.
27. Decaudin D, Brousse N, Brice P, Haioun C, Bourhis J, Morel P, et al. Efficacy of autologous stem cell
transplantation in mantle cell lymphoma: a 3-year follow-up study. Bone Marrow Transplant.
2000;25:251–6.
28. Lenz G, Dreyling M, Hoster E, Wörmann B, Dührsen U, Metzner B, et al. Immunochemotherapy With
Rituximab and Cyclophosphamide, Doxorubicin, Vincristine, and Prednisone Significantly Improves
Response and Time to Treatment Failure, But Not Long-Term Outcome in Patients With Previously
Untreated Mantle Cell Lymphoma: Results of a Prospective Randomized Trial of the German Low
Grade Lymphoma Study Group (GLSG). J Clin Oncol. 2005;23:1984-92.
29. Dreger P, Rieger M, Seyfarth B, Hensel M, Kneba M, Ho AD, et al. Rituximab-Augmented
Myeloablation For First-Line Autologous Stem Cell Transplantation For Mantle Cell Lymphoma:
Effects On Molecular Response And Clinical Outcome. Haematologica. 2007;92:42–9.
30. Thieblemont C, Antal D, Lacotte-Thierry L, Delwail V, Espinouse D, Michallet A, et al. Chemotherapy
with Rituximab Followed by High-Dose Therapy and Autologous Stem Cell Transplantation in Patients
with Mantle Cell Lymphoma. Cancer. 2005;104:1434-41.
31. Schulz H, Bohlius JF, Trelle S, Skoetz N, Reiser M, Kober T, et al. Immunochemotherapy With
Rituximab and Overall Survival in Patients With Indolent or Mantle Cell Lymphoma: A Systematic
Review and Meta-analysis. J Natl Cancer Inst. 2007;99:706-14.
32. Gianni AM, Magni M, Martelli M, Di Nicola M, Carlo-stella C, Pilotti S, et al. Long-term remission in
mantle cell lymphoma following high-dose sequential chemotherapy and in vivo rituximab-purged stem
cell autografting (R-HDS regimen). Blood. 2003;102:749–55.
33. Vose JM. Mantle cell lymphoma : 2017 update on diagnosis, risk-stratification, and clinical
management. Am J Hematol. 2017;92:806–13.
34. Pott C, Hoster E, Delfau-Larue MH, Beldjord K, Böttcher S, Asnafi V, et al. Molecular remission is an
independent predictor of clinical outcome in patients with mantle cell lymphoma after combined
immunochemotherapy: a European MCL intergroup study. Blood. 2010;115:3215–23.
35. Budde LE, Guthrie KA, Till BG, Press OW, Chauncey TR, Pagel JM, et al. Mantle Cell Lymphoma
International Prognostic Index but Not Pretransplantation Induction Regimen Predicts Survival for
Patients With Mantle-Cell Lymphoma Receiving High-Dose Therapy and Autologous Stem-Cell
Transplantation. J Clin Oncol. 2011;29:3023–9.
36. Hoster E, Dreyling M, Klapper W, Gisselbrecht C, Van Hoof A, Kluin-Nelemans HC, et al. A new
prognostic index ( MIPI ) for patients with advanced-stage mantle cell lymphoma. Blood.
2008;111:558–66.
37. Eskelund CW, Kolstad A, Jerkeman M, Räty R, Laurell A, Eloranta S, et al. 15-year follow-up of the
Second Nordic Mantle Cell Lymphoma trial (MCL2): prolonged remissions without survival plateau.
Br J Haematol. 2016;175:410–8.
38. Evens AM, Winter JN, Hou N, Nelson BP, Rademaker A, Patton D, et al. A phase II clinical trial of
intensive chemotherapy followed by consolidative stem cell transplant: long-term follow-up in newly
diagnosed mantle cell lymphoma. Br J Haematol. 2008;140:385–93.
39. Nabhan C, Ragam A, Bitran JD, Mehta J. Hematopoietic SCT for mantle cell lymphoma: is it the
standard of care? Bone Marrow Transplant. 2010;45:1379–87.
40. Younes A, Hilden P, Coiffier B, Hagenbeek A, Salles G, Wilson W, et al. International Working Group
consensus response evaluation criteria in lymphoma (RECIL 2017). Ann Oncol. 2017;28:1436–47.
41. Szcześ niak M, Armatys A, Kurzawa R, Kandzia T, Koziol D, Frankiewicz A, et al. Autologous stem
cell transplantation for mantle cell lymphoma – single centre experience. Contemp Oncol (Pozn).
2013;17:456-9.
42. Laudi N, Arora M, Burns L, Mcglave P, Miller J, Bohac G, et al. Efficacy of High-Dose Therapy and
Hematopoietic Stem Cell Transplantation for Mantle Cell Lymphoma. Am J Hematol. 2006;81:519–24.
43. Armand P, Redd R, Bsat J, Mayuram S, Giardino A, Fisher DC, et al. A phase 2 study of Rituximab-
Bendamustine and Rituximab-Cytarabine for transplant-eligible patients with mantle cell lymphoma. Br
J Haematol. 2016;173(1):89–95.
44. Van ’t Veer MB, de Jong D, MacKenzie M, Kluin-Nelemans HC, van Oers MHJ, Zijlstra J, et al. Highdose
Ara-C and beam with autograft rescue in R-CHOP responsive mantle cell lymphoma patients. Br J
Haematol. 2008;144:524–30.
45. Kolstad A, Laurell A, Jerkeman M, Grønbæk K, Elonen E, Räty R, et al. Nordic MCL3 study: 90 Yibritumomab-
tiuxetan added to BEAM/C in non-CR patients before transplant in mantle cell
lymphoma. Blood. 2014;123:2953–9.
46. Le Gouill S, Thieblemont C, Oberic L, Moreau A, Bouabdallah K, Dartigeas C, et al. Rituximab after
Autologous Stem-Cell Transplantation in Mantle-Cell Lymphoma. N Engl J Med. 2017;377:1250-60.
47. Touzeau C, Leux C, Bouabdallah R, Roussel M, Delarue R, Bouabdallah K, et al. Autologous stem cell
transplantation in mantle cell lymphoma: a report from the SFGM-TC. Ann Hematol. 2014;93(2):233–
42.






