Theranostics in de strijd tegen kanker: twee voor de prijs van een - Karen Leys
De zoektocht naar een nieuw geneesmiddel begint meestal met 1.000.000 moleculen, maar levert slechts één enkel molecuul op dat de race naar de finish overleeft. Tijdens mijn thesis heb ik onderzoek gedaan naar één bepaald molecuul, in de hoop die ‘one in a million’ te vinden.
Het preliminaire onderzoek dat ik voor deze thesis heb uitgevoerd, toonde aan dat het DV1-K-(DV3)-peptide, een stuk van een bepaald eiwit bestaande uit D-aminozuren, een goede vector kan zijn voor bepaalde kankertypes (d.i. een molecuul dat ervoor zorgt dat het gebruikte geneesmiddel naar de juiste plaats in het lichaam gaat). Het gaat daarbij specifiek om kankertypes die de CXCR4-receptor, een soort van sensor, teveel hebben. Het doel is om het DV1-K-(DV3)-peptide op een theranostische wijze in te zetten; het is namelijk een peptide dat als vector zowel kan dienen bij diagnose als bij therapie. Het woord ‘theranostisch’ is dan ook een samenstelling van ‘diagnostisch’ en ‘therapeutisch’. Zo’n aanpak wordt meer en meer gebruikt in de strijd tegen kanker. Net daarom bleek het nuttig om te testen of het DV1-K-(DV3)-peptide een goede vector zou zijn bij deze dubbelzijdige benadering, namelijk bij beeldvorming en behandeling van kanker.
De figuur hierboven (thyroidcancersurvivor; 2010) toont het verschil tussen een normale cel (links) en een abnormale cel of kankercel (rechts). Normale cellen hebben maar enkele receptoren op de buitenrand, terwijl er bij afwijkende cellen teveel receptoren op de buitenrand staan. Dat zorgt ervoor dat stoffen die zich aan de receptoren van kankercellen binden, gebruikt kunnen worden om deze op te sporen en om ze vervolgens te bestrijden. Veel kankertypes hebben te veel CXCR4-receptoren, die bijgevolg een goed doelwit vormen bij het opsporen van tumoren.
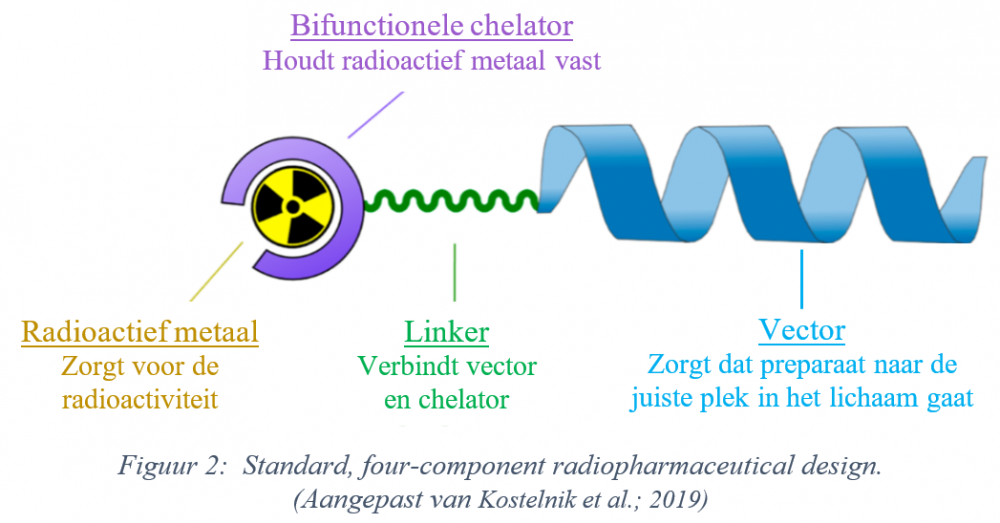
In het Radiopharmaceutical research lab van de K.U. Leuven werd het DV1-K-(DV3)-peptide gebruikt als vector in een radiofarmaceutisch preparaat of ‘tracer’. Die tracer (zie Figuur 2) bevat naast de vector ook een radioactief metaal, een bifunctionele chelator (wat het radioactief metaal vasthoudt) en een linker (een linkend element dat de vector en het geheel van chelator en metaal verbindt). Het gekozen radioactieve metaal bepaalt of het preparaat wordt gebruikt voor beeldvorming (o.a. PET-scans) of therapie; fluor-18 wordt bijvoorbeeld gebruikt bij beeldvorming, actinium-225 dan weer in een therapeutische context. Aangezien eenzelfde vectormolecuul (het DV1-K-(DV3)-peptide) voor zowel beeldvorming als therapie gebruikt kan worden, spreken we over een ‘theranostische’ aanpak.
Mijn werk begon bij het onderzoeken of de vector goed functioneert en enkel bindt waar nodig (op de CXCR4-receptoren). Daarvoor waren meerdere testen nodig met de DV1-K-(DV3)-tracer, die fluor-18 bevat. Fluor-18 werd gebruikt om via een PET-scan de weg te kunnen achterhalen die de radioactieve tracer aflegt in het lichaam, in eerste instantie in muizen en in een volgende fase in kankerpatiënten. Als onderzoeker hoopte ik dat de (gezonde) muizen de tracer relatief snel zouden uitplassen en daarnaast dat die tracer enkel naar de nieren en de blaas zou gaan, zonder zich verder te verspreiden naar andere organen. Bij een muis met een tumor zou de tracer idealiter vooral naar de tumor moeten gaan. Als de tracer in te hoge concentraties terug te vinden is in andere weefsels, dan is hij voor de beoogde organen niet meer bruikbaar, vanwege het gebrek aan contrast tussen normaal weefsel en tumoren.
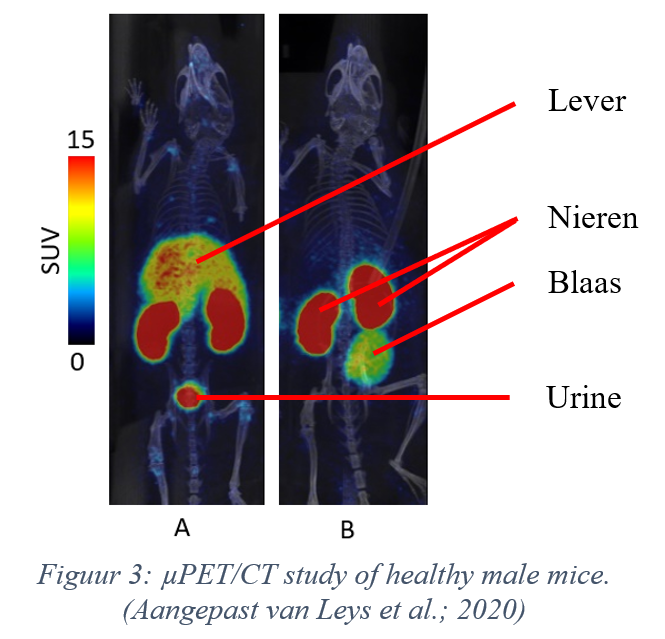
Bovenstaande figuur (Leys et al. 2020) laat zien waar in het lichaam van de onderzochte muizen de tracer zich bevindt, een uur na injectie. Muis A kreeg louter de tracer toegediend, terwijl muis B ook een stof geïnjecteerd kreeg die de CXCR4-receptor blokkeert. Het is gunstig als er aangetoond kan worden dat een tracer enkel en alleen bindt op de beoogde receptor, in dit geval de CXCR4-receptor, en voor deze bijgevolg specifiek is. Hoe specifieker de tracer, hoe beter. Vandaar dat ik, de onderzoeker achter deze thesis, de specifieke status van genoemde tracer bewees, door de binding ervan op de CXCR4-receptor te blokkeren en door vervolgens na te gaan of er nog steeds radioactiviteit aanwezig was in andere organen dan de nieren en de blaas, in dit onderzoek voornamelijk in de lever. Indien er in dit orgaan geen radioactiviteit meer te bespeuren valt, dan was de blokkering succesvol, kan de tracer niet binden en is die dus specifiek. Als er wel nog (in hoge mate) radioactiviteit te vinden is, dan is de tracer niet specifiek en bindt deze niet enkel op de beoogde receptor; de tracer is dan niet bruikbaar. Mijn studie heeft bevestigd dat de DV1-K-(DV3)-tracer specifiek is (zie Figuur 3). Bij muis A vertoont de lever een relatief hoge concentratie aan radioactiviteit; bij muis B (na blokkering) is dat niet meer het geval.
De PET-scan en andere proeven bevestigden dat het DV1-K-(DV3)-peptide als vector goede (farmacokinetische) eigenschappen vertoont (bij muizen). De tracer is namelijk specifiek en verlaat het lichaam op een snelle manier (via de urine). Bovendien is hij bij gezonde muizen enkel zichtbaar in de nieren, de blaas en slechts in mindere mate in de lever, waardoor het contrast in het merendeel van de organen vermoedelijk groot genoeg blijft om tumoren van normaal weefsel te kunnen onderscheiden.
De zoektocht naar een nieuw kankergeneesmiddel is nog lang niet afgerond, maar de besproken tracer lijkt, zij het dan voor de desbetreffende kankertypes, alvast veelbelovend en zou weleens dat ene geneesmiddel kunnen zijn dat de finishlijn haalt.
© Karen Leys
Literatuurlijst
Figuur gebaseerd op thyroidcancersurvivor. What is Cancer? [Internet]. 2010 [geciteerd 18 mei 2020]. Geraadpleegd via: https://thyroidcancersurvivor.wordpress.com/2010/10/13/what-is-cancer/
Figuur gebaseerd op Kostelnik TI, Orvig C. Radioactive Main Group and Rare Earth Metals for Imaging and Therapy. Chem Rev. 2019;119:902–56.
Figuur gebaseerd op Leys K, Bormans G, Cleeren F, Development and preclinical evaluation of new theranostic anti-CXCR4 radiopharmaceuticals. K.U. Leuven; 2020.
Bibliografie
LITERATURE CITED 1. World Nuclear Association. What Is Background Radiation? World Nuclear Association; 2. MedicalNewsToday. What is nuclear medicine? [Internet]. [cited 2020 Mar 5]. Available from: https://www.medicalnewstoday.com/articles/248735 3. Vermeulen K, Vandamme M, Bormans G, Cleeren F. Design and Challenges of Radiopharmaceuticals. Semin Nucl Med. 2019;49(5):339–56. 4. Kostelnik TI, Orvig C. Radioactive Main Group and Rare Earth Metals for Imaging and Therapy. Chem Rev. 2019;119:902–56. 5. Colombetti LG. Principles of radiopharmacology Volume I. 1st ed. Colombetti LG, editor. Boca Raton: CRC press; 1979. 6. Jewett DM, Kilbourn MR. In vivo evaluation of new carfentanil-based radioligands for the mu opiate receptor. Nucl Med Biol. 2004;31:321–5. 7. Science & Technology - Facilities Council. 2. Isotopes and decay - Decay equations [Internet]. [cited 2019 Sep 24]. p. 9. Available from: http://resources.schoolscience.co.uk/stfc/16plus/partich2pg4.html 8. Tro N. 20.4: The Valley of Stability- Predicting the Type of Radioactivity [Internet]. 2019 [cited 2020 Jan 15]. Available from: https://chem.libretexts.org/Bookshelves/General_Chemistry/Map%3A_A_Mole… 0%3A_Radioactivity_and_Nuclear_Chemistry/20.04%3A_The_Valley_of_Stability- _Predicting_the_Type_of_Radioactivity 9. Zalutsky MR, Pruszynski M. Astatine-211: Production and Availability. Curr Radiopharm. 2012;4(3):177–85. 10. Navarro-Teulon I, Lozza C, Pèlegrin A, Vivès E, Pouget JP. General overview of radioimmunotherapy of solid tumors. Immunotherapy. 2013;5(5):467–87. 11. Conti M, Eriksson L. Physics of pure and non-pure positron emitters for PET: A review and a discussion. EJNMMI Phys. 2016;3(8). 12. Scheinberg DA, McDevit MR. Actinium-225 in targeted alpha-particle therapeutic applications. Curr Radiopharm. 2011;4(4):306–20. 13. Kassis AI. Molecular and cellular radiobiological effects of Auger emitting radionuclides. Radiat Prot Dosimetry. 2011;143(2–4):241–7. 14. Strategic Alliance Holdings Global LLC (“SAH Global”). PET & Molecular Imaging [Internet]. [cited 2019 Sep 26]. Available from: https://www.sahglobal.com/pet-molecular-imaging/ 15. Suridjan I, Comley RA, Rabiner EA. The application of positron emission tomography (PET) imaging in CNS drug development. Brain Imaging Behav. 2019;13(2):354–65. 16. Sanchez-Crespo A. Comparison of Gallium-68 and Fluorine-18 imaging characteristics in positron emission tomography. Appl Radiat Isot. 2013;76:55–62. 17. Courses.Washington.edu. How it works: Positron Emission. 18. Connor N. What is Interaction of Beta Radiation with Matter - Definition [Internet]. 2019 [cited 2020 Jan 31]. Available from: https://www.periodic-table.org/what-is-interaction-of-beta-radiation-wi… 19. Fornell D. SPECT Scanner vs. PET, Which is Best? [Internet]. Diagnostic and Interventional Cardiology. 54 2008 [cited 2020 Apr 27]. Available from: https://www.dicardiology.com/article/spect-scanner-vs-petwhich-best 20. Barbalace K. Periodic Table of Elements - Fluorine - F [Internet]. 2019 [cited 2019 Sep 23]. Available from: https://environmentalchemistry.com/yogi/periodic/F.html 21. WebElements. WebElements Periodic Table » Fluorine » the essentials [Internet]. [cited 2019 Sep 23]. Available from: https://www.webelements.com/fluorine/ 22. Christé V, Bé MM, Kuzmenko NK. Fluorine-18 [Internet]. Laboratoire National Henri Becquerel/ CEA. lnhb.fr; [cited 2019 Oct 19]. Available from: http://www.lnhb.fr/nuclear-data/nuclear-data-table/ 23. Cleeren F, Lecina J, Ahamed M, Raes G, Devoogdt N, Caveliers V, McQuade P, Rubins DJ, Li W, Verbruggen A, Xavier C, Bormans G. Al18F-labeling of heat-sensitive biomolecules for positron emission tomography imaging. Theranostics. 2017;7(11):2924–39. 24. Pouget JP, Navarro-Teulon I, Bardiès M, Chouin N, Cartron G, Pèlegrin A, Azria D. Clinical radioimmunotherapy - the role of radiobiology. Nat Rev Clin Oncol. 2011;8(12):720–34. 25. Kassis AI. Molecular and cellular radiobiological effects of Auger emitting radionuclides. Radiat Prot Dosimetry. 2011;143:241–7. 26. Baum RP. Therapeutic Nuclear Medicine [Internet]. 1st ed. Baum RP, editor. Heidelberg: Springer-Verlag Berlin Heidelberg; 2014. (Medical Radiology). Available from: http://link.springer.com/10.1007/978-3- 540-36719-2 27. Barbalace K. Periodic Table of Elements - Lutetium - Lu [Internet]. 2019 [cited 2019 Sep 23]. Available from: https://environmentalchemistry.com/yogi/periodic/Lu.html 28. WebElements. WebElements Periodic Table » Lutetium » the essentials [Internet]. [cited 2019 Sep 23]. Available from: https://www.webelements.com/lutetium/ 29. Barbalace K. Periodic Table of Elements - Actinium - Ac [Internet]. 2019 [cited 2019 Sep 23]. Available from: https://environmentalchemistry.com/yogi/periodic/Ac.html 30. WebElements. WebElements Periodic Table » Actinium » the essentials [Internet]. [cited 2019 Sep 23]. Available from: https://www.webelements.com/actinium/ 31. Deal KA, Davis IA, Mirzadeh S, Kennel SJ, Brechbiel MW. Improved in vivo stability of actinium-225 macrocyclic complexes. J Med Chem. 1999;42:2988–92. 32. Jaggi JS, Kappel BJ, McDevitt MR, Sgouros G, Flombaum CD, Cabassa C, Scheinberg DA. Efforts to control the errant products of a targeted in vivo generator. Cancer Res. 2005;65(11):4888–95. 33. Barbalace K. Periodic Table of Elements - Lanthanum - La [Internet]. 2019 [cited 2019 Sep 23]. Available from: https://environmentalchemistry.com/yogi/periodic/La.html 34. Wilson DJ. What is Theranostics? [Internet]. News Medical Life Sciences. 2018 [cited 2020 Apr 27]. Available from: https://www.news-medical.net/health/What-is-Theranostics.aspx 35. Pene F, Courtine E, Cariou A, Mira J-P. Toward theragnostics. Crit Care Med. 2009;37(SUPPL. 1):S50– 8. 36. Sathekge M. Targeted radionuclide therapy. Contin Med Educ J. 2013;31(8):289–94. 37. Gudkov S V., Shilyagina NY, Vodeneev VA, Zvyagin A V. Targeted radionuclide therapy of human tumors. Int J Mol Sci. 2015;17(1). 38. Hughes CE, Nibbs RJB. A guide to chemokines and their receptors. FEBS J. 2018;285(16):2944–71. 55 39. Kircher M, Herhaus P, Schottelius M, Buck AK, Werner RA, Wester H-JJ, Keller U, Lapa C. CXCR4- directed theranostics in oncology and inflammation. Ann Nucl Med. 2018;32(8):503–11. 40. Bernhagen J, Krohn R, Lue H, Gregory JL, Zernecke A, Koenen RR, Dewor M, Georgiev I, Schober A, Leng L, Kooistra T, Fingerle-Rowson G, Ghezzi P, Kleemann R, McColl SR, Bucala R, Hickey MJ, Weber C. MIF is a noncognate ligand of CXC chemokine receptors in inflammatory and atherogenic cell recruitment. Nat Med. 2007;13(5):587–96. 41. Pawig L, Klasen C, Weber C, Bernhagen J, Noels H. Diversity and Inter-Connections in the CXCR4 Chemokine Receptor/Ligand Family: Molecular Perspectives. Front Immunol. 2015;6(429). 42. The Liotta Research Group, Liotta D. CXCR4 AND CCR5 [Internet]. [cited 2020 Jan 17]. Available from: https://scholarblogs.emory.edu/liotta/projects/cxcr4/ 43. Feng Y, Broder CC, Kennedy PE, Berger EA. HIV-1 Entry Cofactor: Functional cDNA Cloning of a Seven-Transmembrane, G Protein-Coupled Receptor. Science (80- ). 1996;272(5263):872–7. 44. Thackeray JT, Derlin T, Haghikia A, Napp LC, Wang Y, Ross TL, Schäfer A, Tillmanns J, Wester HJ, Wollert KC, Bauersachs J, Bengel FM. Molecular Imaging of the Chemokine Receptor CXCR4 after Acute Myocardial Infarction. JACC Cardiovasc Imaging. 2015;8(12):1417–26. 45. Sun X, Cheng G, Hao M, Zheng J, Zhou X, Zhang J, Taichman RS, Pienta KJ, Wang J. CXCL12 / CXCR4 / CXCR7 chemokine axis and cancer progression. Cancer Metastasis Rev. 2010;29(4):709–22. 46. Tsutsumi H, Tanaka T, Ohashi N, Masuno H, Tamamura H, Hiramatsu K, Araki T, Ueda S, Oishi S, Fujii N. Therapeutic Potential of the Chemokine Receptor CXCR4 Antagonists as Multifunctional Agents. Wiley Intersci. 2007;88(2):279–89. 47. Boulais PE, Dulude D, Cabana J, Heveker N, Escher E, Lavigne P, Leduc R. Photolabeling identifies transmembrane domain 4 of CXCR4 as a T140 binding site. Biochem Pharmacol. 2009;78:1382–90. 48. Wester HJ, Keller U, Schottelius M, Beer A, Philipp-Abbrederis K, Hoffmann F, Šimeček J, Gerngross C, Lassmann M, Herrmann K, Pellegata N, Rudelius M, Kessler H, Schwaiger M. Disclosing the CXCR4 expression in lymphoproliferative diseases by targeted molecular imaging. Theranostics. 2015;5(6):618– 30. 49. Poschenrieder A, Schottelius M, Schwaiger M, Kessler H, Wester HJ. The influence of different metalchelate conjugates of pentixafor on the CXCR4 affinity. EJNMMI Res. 2016;6. 50. George GPC, Pisaneschi F, Nguyen QD, Aboagye EO. Positron emission tomographic imaging of CXCR4 in cancer: challenges and promises. Mol Imaging. 2014;13. 51. Schottelius M, Osl T, Poschenrieder A, Hoffmann F, Beykan S, Hänscheid H, Schirbel A, Buck AK, Kropf S, Schwaiger M, Keller U, Lassmann M, Wester HJ. [177Lu]pentixather: Comprehensive preclinical characterization of a first CXCR4-directed endoradiotherapeutic agent. Theranostics. 2017;7(9):2350–62. 52. Poschenrieder A, Osl T, Schottelius M, Hoffmann F, Wirtz M, Schwaiger M, Wester H. First 18 F-Labeled Pentixafor-Based Imaging Agent for PET Imaging of CXCR4 Expression In Vivo. Tomography. 2016;2(2):85–93. 53. Habringer S, Lapa C, Herhaus P, Schottelius M, Istvanffy R, Steiger K, Slotta-Huspenina J, Schirbel A, Hänscheid H, Kircher S, Buck AK, Götze K, Vick B, Jeremias I, Schwaiger M, Peschel C, Oostendorp R, Wester H-J, Grigoleit G-U et al. Dual Targeting of Acute Leukemia and Supporting Niche by CXCR4- Directed Theranostics. Theranostics. 2018;8(2):369–83. 56 54. Maurer S, Herhaus P, Lippenmeyer R, Hänscheid H, Kircher M, Schirbel A, Maurer CH, Buck AK, Wester H-J, Einsele H, Grigoleit G-U, Keller U, Lapa C. Side effects of CXC-chemokine receptor 4-directed endoradiotherapy with pentixather before hematopoietic stem cell transplantation. J Nucl Med. 2019;60:1399–405. 55. Mao Y, Meng Q, Song P, Zhu S, Xu Y, Snyder EY, An J, Huang Z. Novel Bivalent and D-Peptide Ligands of CXCR4 Mobilize Hematopoietic Progenitor Cells to the Blood in C3H/HeJ Mice. Cell Transplant. 2018;27(8):1249–55. 56. Xu Y, Duggineni S, Espitia S, Richman DD, An J, Huang Z. A synthetic bivalent ligand of CXCR4 inhibits HIV infection. Biochem Biophys Res Commun. 2013;435:646–50. 57. Zhou N, Luo Z, Luo J, Fan X, Cayabyab M, Hiraoka M, Liu D, Han X, Pesavento J, Dong C-Z, Wang Y, An J, Kaji H, Sodroski JG, Huang Z. Exploring the stereochemistry of CXCR4-peptide recognition and inhibiting HIV-1 entry with D-peptides derived from chemokines. J Biol Chem. 2002;277(20):17476–85. 58. Qin L, Kufareva I, Holden LG, Wang C, Zheng Y, Zhao C, Fenalti G, Wu H, Han GW, Cherezov V, Abagyan R, Stevens RC, Handel TM. Crystal structure of the chemokine receptor CXCR4 in complex with a viral chemokine. Science (80- ). 2015;347(6226):1117–22. 59. Zhou N, Luo Z, Luo J, Hall JW, Huang Z. A Novel Peptide Antagonist of CXCR4 Derived from the NTerminus of Viral Chemokine vMIP-II. Biochemistry. 2000;39:3782–7. 60. American Cancer Society. Getting Oral or Systemic Radiation Therapy [Internet]. 2019 [cited 2020 Feb 28]. Available from: https://www.cancer.org/treatment/treatments-and-side-effects/treatmentt… 61. MinFound Medical Systems. PET scanner / CT scanner / for full-body tomography / 16-slice [Internet]. [cited 2020 May 7]. Available from: https://www.medicalexpo.com/prod/minfound-medicalsystems/product-122176… 62. Cleeren F, Lecina J, Bridoux J, Devoogdt N, Tshibangu T, Xavier C, Bormans G. Direct fluorine-18 labeling of heat-sensitive biomolecules for positron emission tomography imaging using the Al18FRESCA method. Nat Protoc. 2018;13(10):2330–47. 63. Suzuki K, Ui T, Nagano A, Hino A, Arano Y. C-terminal–modified LY2510924: a versatile scaffold for targeting C-X-C chemokine receptor type 4. Nat Sci reports. 2019;9(1):1–8. 64. Ucar B. Synthesis and characterization of natural lanthanum labelled DOTA-Peptides for simulating radioactive Ac-225 labeling. Appl Radiat Isot. 2019;153. 65. Schoofs G, Van Hout A, D’huys T, Schols D, Van Loy T. A flow cytometry-based assay to identify compounds that disrupt binding of fluorescently-labeled CXC chemokine ligand 12 to CXC chemokine receptor 4. J Vis Exp. 2018;(e57271). 66. Claes S, D’huys T, Van Hout A, Schols D, Van Loy T. A kinetic fluorescence-based Ca2+ mobilization assay to identify G protein-coupled receptor agonists, antagonists, and allosteric modulators. J Vis Exp. 2018;132. 67. Bergström M, Grahnén A, Långström B. Positron emission tomography microdosing: a new concept with application in tracer and early clinical drug development. p. 357−366. 68. Kinahan PE, Fletcher JW. PET/CT Standardized Uptake Values (SUVs) in Clinical Practice and Assessing Response to Therapy. Natl Inst Heal. 2010;31(6):496–505. 57 69. Fosgerau K, Hoffmann T. Peptide therapeutics: current status and future directions. Drug Discov Today. 2015;20(1):122–8. 70. Meister D, Taimoory SM, Trant JF. Unnatural amino acids improve affinity and modulate immunogenicity: Developing peptides to treat MHC type II autoimmune disorders. Pept Sci. 2019;111. 71. Werner HM, Cabalteja CC, Horne WS. Peptide Backbone Composition and Protease Susceptibility: Impact of Modification Type, Position, and Tandem Substitution. ChemBioChem. 2016;17(8):712–8. 72. Lee AC-L, Harris JL, Khanna KK, Hong J-H. A Comprehensive Review on Current Advances in Peptide Drug Development and Design. Int J Mol Sci. 2019;20(2383). 73. Pike VW. PET Radiotracers: crossing the blood-brain barrier and surviving metabolism. Trends Pharmacol Sci. 2009;30(8):431–40. 74. thyroidcancersurvivor. What is Cancer? [Internet]. 2010 [cited 2020 May 18]. Available from: https://thyroidcancersurvivor.wordpress.com/2010/10/13/what-is-cancer/








