Een aftakelingsproces over de jaren heen
- AmberScheers
Stappatroon- en spierkrachtveranderingen bij ouder wordende kinderen met Duchenne
Ik werd snel moe, viel vaak op de grond en raakte moeilijk terug recht. Mijn ouders werden bezorgd en zo kreeg ik na enkele onderzoeken op driejarige leeftijd de diagnose van een erfelijke en ongeneeslijke spierziekte. Nu, negen jaar later, is wandelen erg moeilijk. Ik weet dat mijn situatie alleen maar zal verergeren en dat ik uiteindelijk in een rolstoel zal terechtkomen.
(Foto © Alexandre Carniato - Pexel)
Dit is het verhaal van Toon, een jongen met de ziekte van Duchenne ofwel Duchenne musculaire dystrofie (DMD). DMD is een aandoening veroorzaakt door een genetisch defect en komt vrijwel enkel voor bij jongens. De ziekte wordt gekenmerkt door spieraantasting en is progressief, wat inhoudt dat de spieren steeds meer verzwakken over de jaren heen. Al op kleuterleeftijd ervaren deze kinderen opvallende wandelmoeilijkheden, wat zich uit in een afwijkende manier van stappen. De ziekte is tot op heden ongeneeslijk en het aftakelingsproces van de spieren tegenhouden is helaas onmogelijk. Meestal wordt men als tiener rolstoelafhankelijk en is de levensverwachting beperkt. Het spreekt dus voor zich dat DMD een ingrijpende aandoening is met ernstige gevolgen. Dit benadrukt de onmisbare nood aan meer wetenschappelijk onderzoek. Eerdere studies hebben ons al veel geleerd, maar kennen een belangrijk tekort. Om de effectiviteit van mogelijk werkzame medicatie te bepalen, is grondige kennis over enerzijds het progressieve ziekteverloop en anderzijds de onderliggende spiermechanismen van het pathologisch gangpatroon essentieel. Als wetenschapper, maar ook als ouder en patiënt zelf, hebben we echter nog steeds geen antwoord op de volgende vragen: “Op welke manier manifesteert het erger wordende stappatroon en de afnemende spierkracht zich bij groeiende jongens met DMD?” en ‘Wat is dan de link tussen hun abnormaal wandelpatroon en spierzwakte?” Hierdoor is het moeilijk om de effecten van behandelingen op de motorische functie en op het behouden van zelfstandig stappen te meten. Dit belemmert uiteindelijk de goedkeuring voor het toedienen van veelbelovende nieuwe medicatie, die de periode van het zelfstandig stappen potentieel kan verlengen.
Wat zijn de veranderingen in het stappatroon en spierkracht in de onderste ledematen?
Op zoek naar antwoorden, exploreerden we de hierboven vermelde vragen binnen het kader van ons twee jaar durend masterthesisproject. Allereerst bestudeerden we hoe het stappatroon en de spierkracht (met de focus op de onderste ledematen) evolueerden over de tijd. Daarvoor voerden we, als een van de eersten ooit, longitudinaal onderzoek uit op een groep van jongens met DMD tijdens het groeiproces. Dit hield in dat ze meermalig onderzocht werden op verschillende tijdstippen. Elk half jaar werden 17 jongens (4 -17 jaar) getest over een totaalperiode van maximaal 18 maanden. Om de gang- en spierkrachtafwijkingen te kwantificeren, werden respectievelijk ganganalyse- en spierkrachtmetingen uitgevoerd. Via ganganalyses werden gegevens over de bewegende gewrichten tijdens het stappen verzameld aan de hand van lichaamssensoren (figuur 1) en camera’s. De spierkracht werd getest in een “krachtstoel” (figuur 2a) met krachtmeter (figuur 2b) door de maximale geleverde spierkracht gedurende vijf tellen te meten.

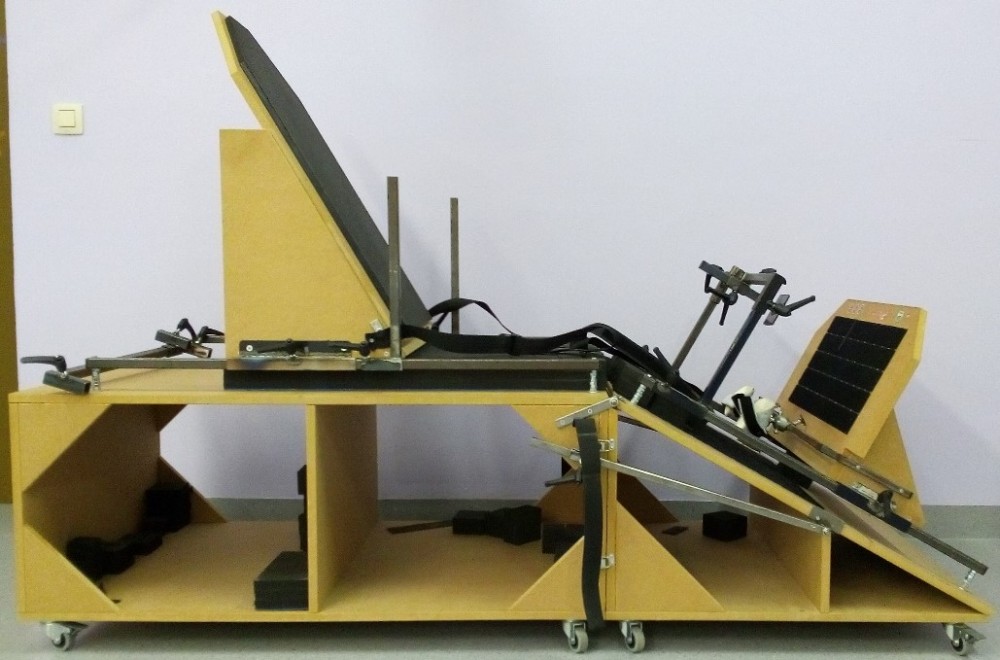

(Van boven naar onder) Fig. 1. Lichaamssensoren om het stappatroon te registeren. - Fig. 2a. “Krachtstoel” om de been- en voetspierkracht te bepalen. - Fig. 2b. Opstelling van de krachtmeter in de “krachtstoel” om de spierkracht van de voetheffers te meten.
Dankzij onze unieke longitudinale analyse konden we aantonen dat bepaalde betekenisvolle gang- en spiersterkteparameters duidelijk achteruitgingen over de tijd. Zo is bijvoorbeeld aangetoond dat het bekken steeds meer voorwaarts kantelt (grafiek 1) - wat een toenemende holle rug heeft als gevolg - en dat de enkelbuigers progressief verzwakken (grafiek 2). Deze verschijnselen zijn niet alleen nuttig om de doeltreffendheid van nieuwe behandelingen na te gaan, maar zijn ook relevante aspecten om op te focussen in therapie, afhankelijk van de noden van het betreffende kind.
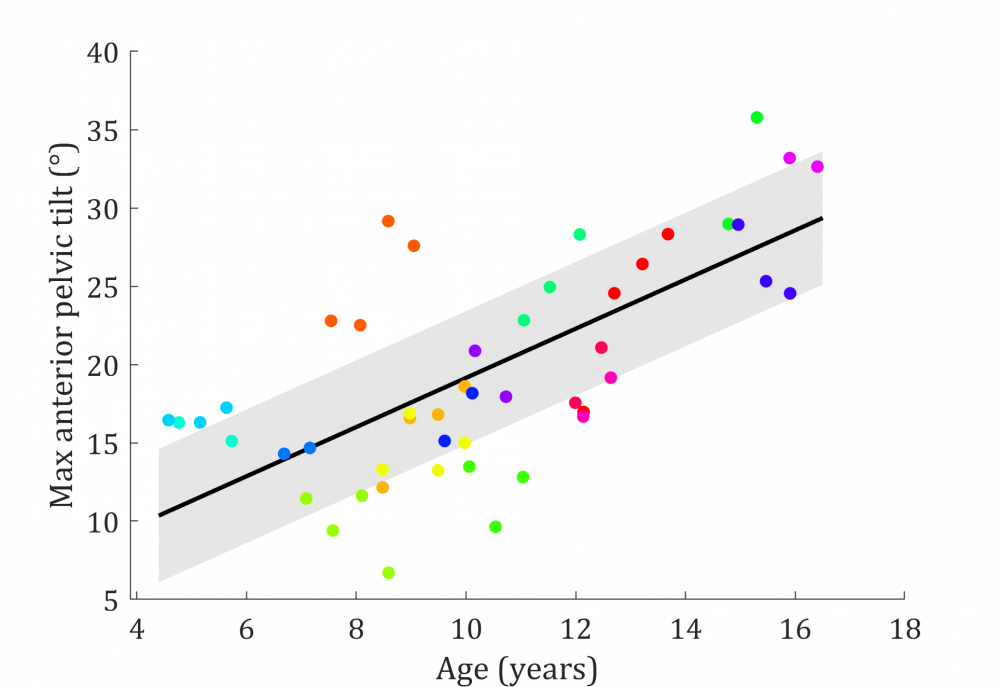
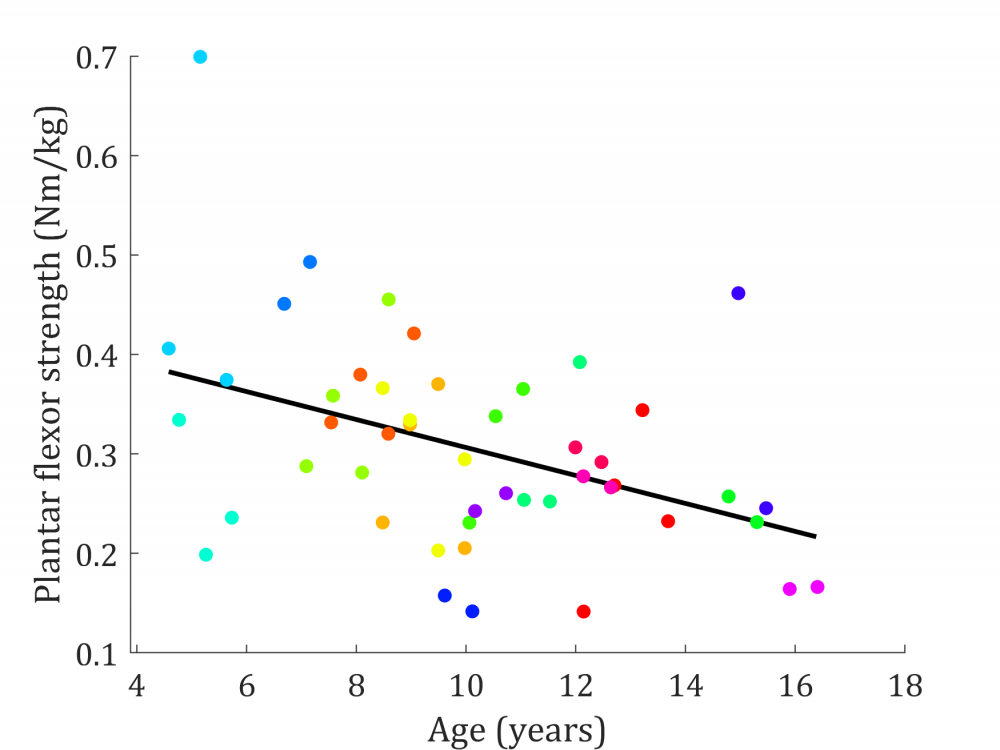
(Van boven naar onder) Grafiek 1. Relatie tussen toenemende leeftijd (age) in jaren (years) op de x-as en de toenemende voorwaartse bekkenkanteling (max anterior pelvic tilt) in graden (°) op de y-as. - Grafiek 2. Relatie tussen toenemende leeftijd (age) in jaren (years) op de x-as en de afnemende enkelbuigerkracht (plantar flexor strength) in Newton meter per kilogram lichaamsgewicht (Nm/kg) op de y-as. (Elke kleur van bolletje komt overeen met een ander kind)
Wat is de link tussen de veranderingen in het stappatroon en zwakte in de onderste ledematen?
Clinici gaan er meestal van uit dat spierzwakte in de onderste ledematen gelinkt is aan het pathologische wandelpatroon bij jongens met DMD. Hoewel dit uiteraard aannemelijk lijkt, blijft het slechts een veronderstelling. De oorsprong van de wandelafwijkingen begrijpen en bewijzen is nochtans waardevol om correcte klinische besluitvorming te optimaliseren en zo de stapmogelijkheden bij deze jongens met DMD zo lang mogelijk te behouden. Bijgevolg werd in deze masterthesis ook een antwoord gezocht op de vraag of we interacties konden aantonen tussen bepaalde gangafwijkingen en spierzwakte in de beenspieren. Onze studie is de eerste die dergelijke associaties tussen beide fenomenen zo grondig heeft kunnen demonstreren. Zo hebben we bijvoorbeeld de link tussen zwakte in de heupstrekkers en een verminderde achterwaartse beenbeweging tijdens steunname kunnen bevestigen, iets wat voorheen louter een vermoeden was (grafiek 3). Deze bekomen resultaten vormen een belangrijke aanzet voor toekomstig onderzoek waarbij onderliggende oorzaken van het afwijkende gangpatroon bij DMD nog uitgebreider verdiept moeten worden.
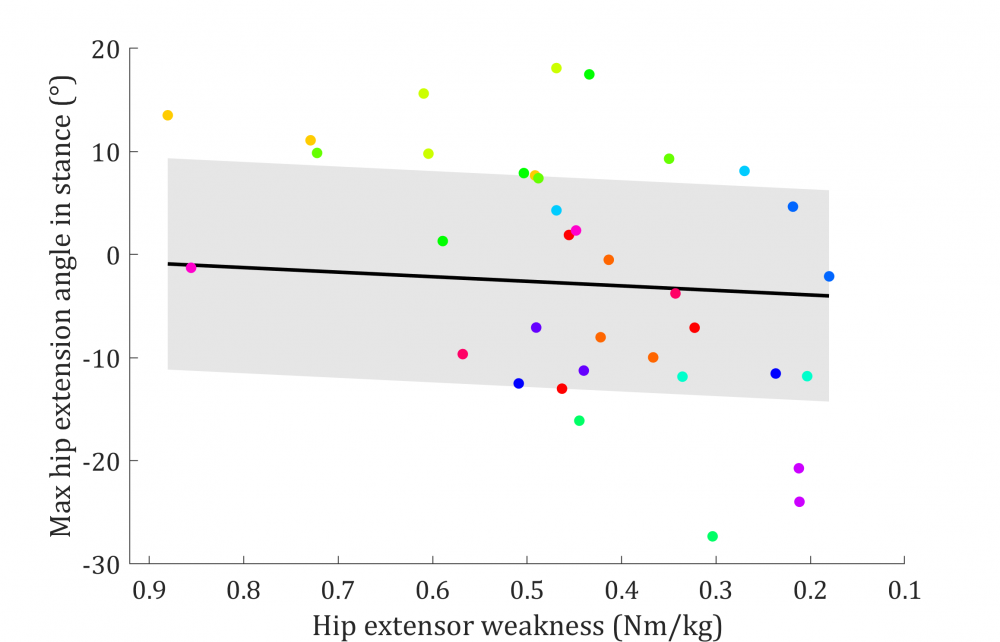
Grafiek 3. Relatie tussen toenemende heupstrekkerzwakte (hip extensor weakness) in Newton meter per kilogram lichaamsgewicht (Nm/kg) op de x-as en afnemende heupstrekhoek tijdens steunname (max hip extension angle in stance) in graden (°) op de y-as. (Elke kleur van bolletje komt overeen met een ander kind)
Een blik op de toekomst
Met de nieuwe inzichten van onze masterproef dragen we bij aan de huidige kennis over het progressief afwijkende gangpatroon en de toenemende spierzwakte, en de onderliggende spiermechanismes van de gangproblematiek bij jongens met DMD. De verworven resultaten kunnen dienen als uitgangspunt voor toekomstig onderzoek naar de ziekteprogressie en kunnen helpen bij het testen van nieuwe medicatie en behandelingen. Op die manier kunnen we in de toekomst jongens zoals Toon hopelijk de kans geven om langer zelfstandig te stappen.
Bibliografie
[1] E.B. Patte K, Pélissier J, Bénaim C, Laassel E, Guibal C, Analyse de la marche au cours de la dystrophie musculaire de Duchenne, Ann Readapt Med Phys. 43 (2000) 57–68.
[2] M. Sussman, Duchenne Muscular Dystrophy, (2002) 138–151.
[3] P.T. Boekhold KJ, Rosenblatt JD, Aging normal and dystrophic mouse muscle: Analysis of myogenicity in cultures of living single fibers, Muscle Nerve. 21 (1998) 173–83.
[4] E. Hoffmann E. Dystrophinopathies. In: Karpati G, Hilton-Jones D, Griggs R, Disorders of Voluntary Muscle, Cambridge, UK Cambridge Univ. Press. (2001) 385–432.
[5] J.P. Infante, V.A. Huszagh, Mechanisms of resistance to pathogenesis in muscular dystrophies, (1999) 155–167.
[6] K.L. Darras BT, Menache-Starobinski CC, Hinton V, Neuromuscular Disorders of Infancy, Childhood, and Adolescence A Clinicians Approach, 2nd edn, Dystrophinopathies. Chapter 30. Darras BT, Jones H, Ryan M, Vivo DC, Eds. (2015) 551–92.
[7] F. Emery, A.; Muntoni, Duchenne muscular dystrophy, 3. Oxford Oxford Univ. Press. (2003).
[8] R.M. Bendixen, D.J. Lott, C. Senesac, S. Mathur, K. Vandenborne, Participation in daily life activities and its relationship to strength and functional measures in boys with Duchenne muscular dystrophy, Disabil. Rehabil. 36 (2014) 1918–1923. doi:10.3109/09638288.2014.883444.
[9] Y. Ishikawa, Duchenne muscular dystrophy, Thorax. 54 (1999) 562–562. doi:10.1007/s10295-005-0227-0.
[10] R.T. Moxley, S. Pandya, E. Ciafaloni, D.J. Fox, K. Campbell, Change in natural history of Duchenne muscular dystrophy with long-term corticosteroid treatment: Implications for management, J. Child Neurol. 25 (2010) 1116–1129. doi:10.1177/0883073810371004.
[11] E. Mazzone, D. Martinelli, A. Berardinelli, S. Messina, A. D’Amico, G. Vasco, E. Al, North Star Ambulatory Assessment, 6-minute walk test and timed items in ambulant boys with Duchenne muscular dystrophy, Neuromuscul. Disord. 20 (2010) 712–716. doi:10.1016/j.nmd.2010.06.014.
[12] A. Berardinelli, M. Scutifero, G. Vasco, A. Sacco, L. Doglio, L. Politano, E. Al, Functional
33
changes in Duchenne muscular dystrophy: A 12-month longitudinal cohort study, Neurology. 77 (2011) 250–256. doi:10.1212/wnl.0b013e318225ab2e.
[13] C.M. McDonald, E.K. Henricson, J.J. Han, R.T. Abresch, A. Nicorici, G.L. Elfring, L. Atkinson, A. Reha, S. Hirawat, L.L. Miller, The 6-minute walk test as a new outcome measure in duchenne muscular dystrophy, Muscle and Nerve. 41 (2010) 500–510. doi:10.1002/mus.21544.
[14] M. Kierkegaard, A. Tollbäck, Reliability and feasibility of the six minute walk test in subjects with myotonic dystrophy, Neuromuscul. Disord. 17 (2007) 943–949. doi:10.1016/j.nmd.2007.08.003.
[15] A.E. Lammers, A.A. Hislop, Y. Flynn, S.G. Haworth, The 6-minute walk test: Normal values for children of 4-11 years of age, Arch. Dis. Child. 93 (2008) 464–468. doi:10.1136/adc.2007.123653.
[16] S. Frosini, G. Vita, T. Mongini, L. Politano, L. Bello, G. Astrea, E. Al, Reliability of the North Star Ambulatory Assessment in a multicentric setting, Neuromuscul. Disord. 19 (2009) 458–461. doi:10.1016/j.nmd.2009.06.368.
[17] C.G. McDonald CM, Abresch RT, Profiles of neuromuscular diseases. Duchenne muscular dystrophy., J. Phys. Med. Rehabil. 74 (1995) 70–92.
[18] L. Doglio, E. Pavan, I. Pernigotti, P. Petralia, C. Frigo, C. Minetti, Early signs of gait deviation in Duchenne muscular dystrophy, Eur. J. Phys. Rehabil. Med. 47 (2011) 587–594.
[19] K. Heberer, E. Fowler, L. Staudt, S. Sienko, C.E. Buckon, A. Bagley, M. Sison-Williamson, C.M. McDonald, M.D. Sussman, Hip kinetics during gait are clinically meaningful outcomes in young boys with Duchenne muscular dystrophy, Gait & Posture. 48 (2016) 159–164. doi:10.1016/j.gaitpost.2016.05.013.
[20] N. Goemans, M. van den Hauwe, R. Wilson, A. van Impe, K. Klingels, G. Buyse, Ambulatory capacity and disease progression as measured by the 6-minute-walk-distance in Duchenne muscular dystrophy subjects on daily corticosteroids, Neuromuscul. Disord. 23 (2013) 618–623. doi:10.1016/j.nmd.2013.05.006.
[21] T.A.L. Wren, G.E. Gorton, S. Õunpuu, C.A. Tucker, Efficacy of clinical gait analysis: A systematic review, Gait& Posture. 34 (2011) 149–153. doi:10.1016/j.gaitpost.2011.03.027.
[22] R. EK, Muscular dystrophy, Pediatr Rev. 21(7) (2000) 233–7.
34
[23] P.S. David H. Sutherland, Richard Olshen, Les Cooper, Marilynn Wyatt, Judy Leach, Scott Mubarak, The pathomechanics of gait in Duchenne Muscular Dystrophy, Dev. Med. Child Neurol. 23 (1981) 3–22.
[24] J.D. Hsu, J.B.S. Furumasu, Gait and Posture Changes in the Duchenne Muscular Dystrophy Child, Clin. Orthop. Relat. Res. March 1993. (1993).
[25] P.J. Khodadadeh S, McClelland MR, Variations of gait parameters in Duchenne muscular dystrophy, Proc Inst Mech Eng [H]. 204(4) (1990) 241–3.
[26] F.A. Frigo C, Licari V, Assessment of gait in muscular dystrophy based on biomechanical analysis, Jonhson BE, Ed. Biomech. X-A. Champaign Hum. Kinet. Publ. (1997).
[27] M.G. D’Angelo, M. Berti, L. Piccinini, M. Romei, M. Guglieri, S. Bonato, A. Degrate, A.C. Turconi, N. Bresolin, Gait pattern in Duchenne muscular dystrophy, Gait & Posture. 29 (2009) 36–41. doi:10.1016/j.gaitpost.2008.06.002.
[28] S.G. Boccardi S, Gabardi C, Negrini A, Locomotor and posture strategies in patients with Duchenne muscular dystrophy (DMD). Part I. Gait analysis, Eur Med Phys. 33 (1997) 13–22.
[29] N. Gaudreault, D. Gravel, S. Nadeau, S. Houde, D. Gagnon, Gait patterns comparison of children with Duchenne muscular dystrophy to those of control subjects considering the effect of gait velocity, Gait & Posture. 32 (2010) 342–347. doi:10.1016/j.gaitpost.2010.06.003.
[30] M. Goudriaan, M. Van den Hauwe, J. Dekeerle, L. Verhelst, G. Molenaers, N. Goemans, K. Desloovere, Gait deviations in Duchenne muscular dystrophy—Part 1. A systematic review, Gait & Posture. 62 (2018) 247–261. doi:10.1016/j.gaitpost.2018.03.020.
[31] M. Goudriaan, M. Van Den Hauwe, C. Simon-martinez, C. Huenaerts, G. Molenaers, N. Goemans, K. Desloovere, Gait & Posture Gait deviations in Duchenne muscular dystrophy — Part 2 . Statistical non- parametric mapping to analyze gait deviations in children with Duchenne muscular dystrophy, Gait & Posture. 63 (2018) 159–164. doi:10.1016/j.gaitpost.2018.04.038.
[32] R. DA Marden FA, Connolly AM, Siegel MJ, Compositional analysis of muscle in boys with Duchenne muscular dystrophy using MR imaging, Skelet. Radiol. 34 (2005) 40–8.
[33] M.F. Nunes, M.E. Hukuda, F.M. Favero, A.B. Oliveira, M.C. Voos, Relationship between
35
muscle strength and motor function in Duchenne muscular dystrophy, (2016) 530–535. doi:10.1590/0004-282X20160085.
[34] S. Mathur, D.J. Lott, C. Senesac, S.A. Germain, R.S. Vohra, H.L. Sweeney, G.A. Walter, K. Vandenborne, Age-Related Differences in Lower-Limb Muscle Cross-Sectional Area and Torque Production in Boys With Duchenne Muscular Dystrophy, Arch. Phys. Med. Rehabil. 91 (2010) 1051–1058. doi:10.1016/j.apmr.2010.03.024.
[35] J.E. Mayhew, J.M. Florence, T.P. Mayhew, E.K. Henricson, R.T. Leshner, R.J. McCarter, D.M. Escolar, Reliable surrogate outcome measures in multicenter clinical trials of Duchenne muscular dystrophy, Muscle and Nerve. 35 (2007) 36–42. doi:10.1002/mus.20654.
[36] B. RW, Manual muscle testing: does it meet the standards of an adequate screening test?, Clin. Rehabil. 19 (2005) 662–667. http://search.ebscohost.com/login.aspx?direct=true&db=ccm&AN=106393590&….
[37] S. W.A., M. W.K., Reliability of quantitative muscle testing in healthy children and in children with Duchenne muscular dystrophy using a hand-held dynamometer, Phys. Ther. 68 (1988) 977–982.
[38] A. Lerario, S. Bonfiglio, M. Sormani, A. Tettamanti, S. Marktel, S. Napolitano, E. Al, Quantitative muscle strength assessment in duchenne muscular dystrophy : longitudinal study and correlation with functional measures, (2012).
[39] C. Buckon, S. Sienko, A. Bagley, M. Sison-Williamson, E. Fowler, L. Staudt, E. Al, Can quantitative muscle strength and functional motor ability differentiate the influence of age and corticosteroids in ambulatory boys with duchenne muscular dystrophy?, PLoS Curr. 8 (2016). http://www.plos.org/publications/currents/%0Ahttp://ovidsp.ovid.com/ovi….
[40] D. O. M. Scott MCSP Mrs. S. A. Hyde MCSP C. Goddard MCSP Dr. V. Dubowitz MD, FRCP, Quantitation of muscle function in children: a prospective study in Duchenne muscular dystrophy., Muscle and Nerve. 5 (1982) 291–301.
[41] H. Akima, D. Lott, C. Senesac, J. Deol, S. Germain, I. Arpan, R. Bendixen, H. Lee Sweeney, G.
36
Walter, K. Vandenborne, Relationships of thigh muscle contractile and non-contractile tissue with function, strength, and age in boys with Duchenne muscular dystrophy, Neuromuscul. Disord. 22 (2012) 16–25. doi:10.1016/j.nmd.2011.06.750.
[42] M.R. Pierrynowski, V. Galea, Enhancing the ability of gait analyses to differentiate between groups: Scaling gait data to body size, Gait & Posture. 13 (2001) 193–201. doi:10.1016/S0966-6362(01)00097-2.
[43] L. Hof, Scaling data to body size, Gait & Posture. 4 (1996) 222–223.
[44] R. Baker, J.L. Mcginley, M.H. Schwartz, S. Beynon, A. Rozumalski, H.K. Graham, O. Tirosh, The Gait Profile Score and Movement Analysis Profile, Gait & Posture. 30 (2019) 265–269. doi:10.1016/j.gaitpost.2009.05.020.
[45] M. Angélica, D. Souza, A. Cezarani, E. Aparecida, G. Barroso, D.Q. Davoli, S. Márcia, R. Jones, A.C. Mattiello-sverzut, The use of the gait profile score and gait variable score in individuals with Duchenne Muscular Dystrophy, 98 (2020). doi:10.1016/j.jbiomech.2019.109485.
[46] N. Gaudreault, D. Gravel, S. Nadeau, Evaluation of plantar flexion contracture contribution during the gait of children with Duchenne muscular dystrophy, J. Electromyogr. Kinesiol. 19 (2009) e180–e186. doi:10.1016/j.jelekin.2007.09.004.
[47] R. Ganea, P.Y. Jeannet, A. Paraschiv-Ionescu, N.M. Goemans, C. Piot, M. Van Den Hauwe, K. Aminian, Gait assessment in children with duchenne muscular dystrophy during long-distance walking, J. Child Neurol. 27 (2012) 30–38. doi:10.1177/0883073811413581.
[48] M. Goudriaan, A. Nieuwenhuys, S.H. Schless, N. Goemans, G. Molenaers, K. Desloovere, A new strength assessment to evaluate the association between muscle weakness and gait pathology in children with cerebral palsy, PLoS One. 13 (2018) 1–22. doi:10.1371/journal.pone.0191097.
[49] Y.B.Y. Hochberg, Controlling the False Discovery Rate: A Practical and Powerful Approach tp multiple testing, J. R. Stat. Soc. Ser. B. 57 (1995) 289–300.
[50] S. Rabe-Hesketh, A. Skrondal, A. Pickles, Reliable Estimation of Generalized Linear Mixed Models using Adaptive Quadrature, Stata J. Promot. Commun. Stat. Stata. 2 (2002) 1–21. doi:10.1177/1536867x0200200101.
[51] J.A. McCullagh, P, & Nelder, Generalized Linear Models, 2nd ed., Chapman & Hall/CRC Press., 1989.
37
[52] H. Goldstein, Multilevel Statistical Models, London, 1995.
[53] J.M.N. Charles E. McCulloch, Shayle R. Searle, Generalized, Linear, and Mixed Models, John Wiley & Sons, New York, 2001.
[54] R.J. Snijders, T. A. B. & Bosker, Multilevel Analysis: An Introduction to Basic and Advanced Multilevel Modeling, 2nd ed., SAGE Publications, 2012.
[55] B.J. Babin, R.E. Anderson, Multivariate Data Analysis, 2006.
[56] K.P. Burnham, D.R. Anderson, Multimodel inference: Understanding AIC and BIC in model selection, Sociol. Methods Res. 33 (2004) 261–304. doi:10.1177/0049124104268644.
[57] I.J. Myung, Tutorial on maximum likelihood estimation, J. Math. Psychol. 47 (2003) 90–100. doi:10.1016/S0022-2496(02)00028-7.
[58] van der H.J. Beenakker EA, Maurits NM, Fock JM, Brouwer OF, Functional ability and muscle force in healthy children and ambulant Duchenne muscular dystrophy patients, Eur J Paediatr Neurol. 9 (2005) 387–93.
[59] R.U. Parreira SL, Resende MB, Della Corte Peduto M, Marie SK, Carvalho MS, Quantification of muscle strength and motor ability in patients with Duchenne muscular dystrophy on steroid therapy., Arq Neuropsiquiatr. 65 (2007) 245–50.
[60] B.K. Krautwurst, S.I. Wolf, D.W.W. Heitzmann, S. Gantz, F. Braatz, T. Dreher, The influence of hip abductor weakness on frontal plane motion of the trunk and pelvis in patients with cerebral palsy, Res. Dev. Disabil. 34 (2013) 1198–1203. doi:10.1016/j.ridd.2012.12.018.
[61] E.M. Gutierrez, Å. Bartonek, Y. Haglund-Åkerlind, H. Saraste, Kinetics of compensatory gait in persons with myelomeningocele, Gait & Posture. 21 (2005) 12–23. doi:10.1016/j.gaitpost.2003.11.002.
[62] C.R.J. a Baptista, A. a Costa, T.M. Pizzato, F.B. Souza, A.C. Mattiello-Sverzut, Postural alignment in children with Duchenne muscular dystrophy and its relationship with balance., Brazilian J. Phys. Ther. 18 (2013) 119–26. doi:10.1590/S1413-35552012005000152.
[63] S. Armand, M. Mercier, E. Watelain, K. Patte, J. Pelissier, F. Rivier, A comparison of gait in spinal muscular atrophy, type II and Duchenne muscular dystrophy, Gait & Posture. 21 (2005) 369–378. doi:10.1016/j.gaitpost.2004.04.006.
38
[64] N.C. K. Uchikawa, M. Liu, K. Hanayama, T. Tsuji, T. Fujiwara, Functional status and muscle strength in people with Duchenne muscular dystrophy living in the community, J. Rehabil. Med. 36 (2004).
[65] G.J.L. J.P. Bakker, I.J. de Groot, A. Beelen, Predictive Factors of Cessation of Ambulation in Patients with Duchenne Muscular Dystrophy Project motion Controlled Arm Support, McArm View project Outcome Measures for Mitochondrial Disease View project, Am. J. Phys. Med. Rehabil. 81 (2003).
[66] B. Palmieri, V. Sblendorio, A. Ferrari, A. Pietrobelli, Duchenne muscle activity evaluation and muscle function preservation: Is it possible a prophylactic strategy?, Obes. Rev. 9 (2008) 121–139. doi:10.1111/j.1467-789X.2007.00423.x.
[67] V. Tiffreau, F. Leboeuf, M. Lempereur, Y. Pereon, S. Brochard, S. Peudenier, Y. Delpierre, L. Delporte, R. Gross, C. Vuillerot, J. Ropars, J.-M. Cuisset, Muscle Activation during Gait in Children with Duchenne Muscular Dystrophy, PLoS One. 11 (2016) e0161938. doi:10.1371/journal.pone.0161938.
[68] A.C. Fry, C.C. Irwin, J.X. Nicoll, D.E. Ferebee, Muscular strength and power in 3- To 7-year-old children, Pediatr. Exerc. Sci. 27 (2015) 345–354. doi:10.1123/pes.2014-0152.
[69] A. Moraux, A. Canal, G. Ollivier, I. Ledoux, V. Doppler, C. Payan, J.Y. Hogrel, Ankle dorsi- and plantar-flexion torques measured by dynamometry in healthy subjects from 5 to 80 years, BMC Musculoskelet. Disord. 14 (2013). doi:10.1186/1471-2474-14-104.
[70] V.L. Chester, M. Tingley, E.N. Biden, A comparison of kinetic gait parameters for 3 – 13 year olds, Clin. Biomech. 21 (2006) 726–732. doi:10.1016/j.clinbiomech.2006.02.007.
[71] F.T. Kanehisa H, Ikegawa S, Tsunoda N, Strength and crosssectional areas of reciprocal muscle groups in the upper arm and thigh during adolescence, Int. J. Sports Med. 16 (1995).
[72] P.A. Ounpuu, S., Davis, R.B., DeLuca, Three-dimensional lower extremity joint kinetics in normal pediatric gait., J. Pediatr. Orthop. 11 (1991) 341–349.
[73] et al. Cupp, T., Oeffinger, D., Tylkowski, C., Age-related kinetic changes in normal pediatrics., J. Pediatr. Orthop. 19 (1999) 475–478.
[74] E.M. Yiu, A.J. Kornberg, Duchenne muscular dystrophy, 51 (2015) 759–764. doi:10.1111/jpc.12868.
39
[75] P. Lasko-mccarthey, Kinematic Variability and Relationships Characterizing the Development of Walking, Dev. Psychobiolcigy. 23 (1990) 809–837.
[76] W.M. Sutherland DH, Olshen RA, Biden EN, The Development of Mature Walking, MacKeith Press, London, 1988.
[77] T.C. B. Balaban, D.J. Matthews, G.H. Clayton, Corticosteroid treatment and functional improvement in Duchenne muscular dystrophy: long-term effect, Am. J. Phys. Med. Rehabil. 84 (2005) 843–850.
[78] J.P.M. J.R. Mendell, R.T. Moxley, R.C. Griggs, M.H. Brooke, G.M. Fenichel, E. Al., Randomized, double-blind six-month trial of prednisone in Duchenne’s muscular dystrophy, N. Engl. J. Med. 1989 (320AD) 592–1597.
[79] C. Angelini, The role of corticosteroids in muscular dystrophy: a critical appraisal, Muscle Nerve. 36 (2007) 424–435.







