
Als je lever én je nieren ziek zijn, wat dan?
Vijf uur ’s ochtends, ik word opgebeld door de transplantcoördinator van UZ Leuven. Neen, ik sta niet op de wachtlijst voor een transplantatie, gelukkig. Met spoed haast ik me naar Gasthuisberg. Met nog grotere spoed en zwaailichten rijden we naar Oostende. Daar beleef ik live voor het eerst een operatie bij een overleden vrouw. Haar organen zullen een nieuwe bestemming krijgen en het leven redden van iemand anders. De lever en één van de nieren gaan samen naar Leuven voor een gecombineerde lever-niertransplantatie.
Niet één maar twee organen falen
Een transplantatie is tegenwoordig een veelvoorkomende operatie bij patiënten waarbij een orgaan faalt. Sinds 20 jaar worden er, naast enkelvoudige lever- of niertransplantaties, ook gecombineerde lever- en niertransplantaties uitgevoerd in UZ Leuven. Dit is een levensreddende behandeling voor patiënten waarbij zowel de lever als de nier faalt. Door de lange wachtlijst voor een transplantatie is het belangrijk om een grondige overweging te maken voor een gecombineerde lever‑niertransplantatie (ten opzichte van alleen een lever- of niertransplantatie). Momenteel is er weinig kennis over de complicaties en overleving na deze operatie. Daarom trachtte ik tijdens mijn masterthesis een antwoord te vinden op volgende vragen. Wat zijn de meest voorkomende redenen voor een gecombineerde lever-niertransplantatie? Wat zijn de overlevingskansen na een gecombineerde lever-niertransplantatie? Ervaren patiënten na een gecombineerde lever‑niertransplantatie meer en ernstigere complicaties ten opzichte van patiënten met alleen een levertransplantatie?
Met deze info hoopt UZ Leuven een beter inzicht te krijgen op mogelijke problemen na dergelijke transplantatie en de kwaliteit van haar zorgprogramma te verbeteren.
Waarom een transplantatie?
We stelden vast dat vooral patiënten met cystes op zowel lever als nieren (polycystische lever- en nierziekte) een gecombineerde lever-niertransplantatie ondergaan. Hierbij werken de lever en nieren nog deels maar hebben zij een erg grote omvang door de vele cystes (het orgaan kan tot 10 kg wegen). De grootte en het gewicht van deze zieke organen zorgen voor heel wat complicaties bij de patiënt.
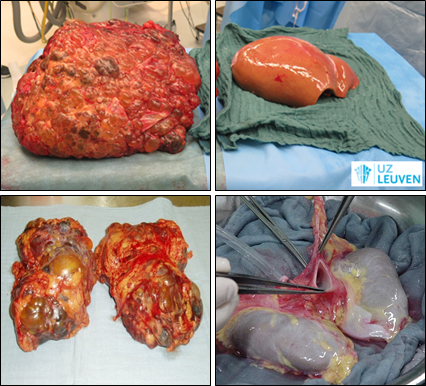
De bovenstaande afbeeldingen tonen een polycystische lever met daarnaast een gezonde lever. Onderaan zijn polycystische nieren met daarnaast gezonde nieren weergegeven.
Overleving na transplantatie
Uit deze thesis is gebleken dat zowel de patiëntoverleving als de overleving van de nieuwe lever en nier, de eerste vijf jaar na de transplantatie, vergelijkbaar of mogelijks zelfs beter waren dan de resultaten uit studies van andere ziekenhuizen. Zelfs wanneer we onze gecombineerde lever‑niertransplantatiepopulatie vergelijken met levertransplantatiepatiënten of niertransplantatiepatiënten in UZ Leuven waren de resultaten gelijkaardig of vermoedelijk beter. Helaas waren er noch in onze studie noch in de literatuur voldoende gegevens beschikbaar over de overleving tien jaar na de operatie om betrouwbare lange-termijnconclusies te trekken.
Complicaties na transplantatie
Uit dit onderzoek komt naar voren dat er meer complicaties optreden bij patiënten die een gecombineerde lever-niertransplantatie ondergaan in vergelijking met patiënten die een enkelvoudige levertransplantatie ondergaan.
Vooral het aantal minder ernstige complicaties (bijvoorbeeld bacteriële of virale infecties) was hoger in de gecombineerde groep. Een mogelijke oorzaak hiervoor is de medicatie die de patiënt nodig heeft na een transplantatie. De dosis van deze medicatie is namelijk hoger na een gecombineerde transplantatie dan na een enkelvoudige transplantatie.
Het aantal ernstige complicaties (bijvoorbeeld bloedingen aan lever of nier, falen van het nieuwe orgaan of kanker) daarentegen waren gelijkaardig in beide groepen.
Evoluties over 20 jaar
De afgelopen 20 jaar is het verblijf op intensieve zorgen na een gecombineerde transplantatie opmerkelijk langer geworden. We vonden nog geen duidelijke verklaringen voor deze stijging. Al vermoeden we dat de steeds oudere, ziekere en zwakkere patiëntenpopulatie hier mee verantwoordelijk voor is. Maar de beschikbare data ondersteunen deze stelling onvoldoende. Daarom wil UZ Leuven in de toekomst gegevens bijhouden over de spierafbraak en over de algemene zwakte van de patiënten. We vermoeden dat deze, naast een aantal lever- en nierspecifieke parameters, een goede algemene indruk kunnen geven over de toestand van de patiënt op het moment van transplantatie.
De essentie?
Mijn masterthesis vormt een klein puzzelstukje in het steeds verder evoluerend medisch onderzoek met als doel meer levenskansen te creëren voor patiënten. Met deze thesis heeft UZ Leuven alvast hoopgevende informatie over de gecombineerde transplantatie van lever en nier.
Naast de interessante resultaten onderzocht tijdens mijn masterthesis is me vooral de dankbaarheid van de patiënten bijgebleven. Sommige patiënten waren doodziek voor hun transplantatie. Wanneer ze enkele weken later met nieuwe organen, nieuwe moed en een stralende glimlach naar huis gaan, fleurde de hele transplantatie-afdeling even op!
Bibliografie
Bibliography
1. Ruiz R, Kunitake H, Wilkinson AH, Danovitch GM, Farmer DG, Ghobrial RM, et al. Long-term analysis of combined liver and kidney transplantation at a single center. Arch Surg. 2006;141(8):735–41.
2. Nadim MK, Sung RS, Davis CL, Andreoni KA, Biggins SW, Danovitch GM, et al. Simultaneous liver-kidney transplantation summit: Current state and future directions. Am J Transplant. 2012;12(11):2901–8.
3. Busuttil RW, Farmer DG, Yersiz H, Hiatt JR, McDiarmid S V., Goldstein LI, et al. Analysis of long-term outcomes of 3200 liver transplantations over two decades: A single-center experience. Ann Surg. 2005;241(6):905–18.
4. Martin E, Huang J, Qun X, Klein J, Bajaj J, Saeian K. Recipient survival and graft survival are not diminished by simultaneous liver-kidney transplantation: an analysis of the United Network for Organ Sharing Database. Liver Transplant. 2012;18:914–29.
5. Coquillard C, Berger J, Daily M, Shah M, Mei X, Marti F, et al. Combined liver–kidney transplantation for polycystic liver and kidney disease: analysis from the United Network for Organ Sharing dataset. Liver Int. 2016;36(7):1018–25.
6. Raad voor transplantatie UZ Leuven. Zorgprogramma Levertransplantatie. Jaarverslag. 2018.
7. Ekser B, Mangus RS, Kubal CA, Powelson JA, Fridell JA, Goggins WC. Excellent outcomes in combined liver-kidney transplantation: Impact of kidney donor profile index and delayed kidney transplantation. Liver Transplant. 2018;24(2):222–32.
8. Wiesner R, Edwards E, Freeman R, Harper A, Kim R, Kamath P, et al. Model for end-stage liver disease (MELD) and allocation of donor livers. Gastroenterology. 2003;124(1):91–6.
9. Abdel-Misih SRZ, Bloomston M. Liver Anatomy. Surg Clin North Am. 2010;90(4):643–53.
10. Steelandt B. Monitoring van morbiditeit en mortaliteit na levertransplantatie ter vrijwaring van veiligheid en kwaliteit. 2019.
11. Liver histology [Internet]. [cited 2020 Feb 4]. Available from: https://www.kenhub.com/en/library/anatomy/liver-histology%0D
12. Trefts E, Gannon M, Wasserman DH. The liver. Curr Biol. 2017;27(21):R1147–51.
13. Wang H, Liang X, Gravot G, Thorling CA, Crawford DHG, Xu ZP, et al. Visualizing liver anatomy, physiology and pharmacology using multiphoton microscopy. J Biophotonics. 2017;10(1):46–60.
14. Gallbladder [Internet]. 16 jan. 2020 [cited 2020 Feb 22]. Available from: https://academic-eb-com.kuleuven.ezproxy.kuleuven.be/levels/collegiate/…
15. Gordillo M, Evans T, Gouon-Evans V. Orchestrating liver development. Dev. 2015;142(12):2094–108.
16. Burra P, Burroughs A, Graziadei I, Pirenne J, Valdecasas JC, Muiesan P, et al. EASL Clinical Practice Guidelines: Liver transplantation. J Hepatol. 2016;64(2):433–85.
17. Bonsib SM. Atlas of Medical Renal Pathology. Atlas Med Ren Pathol. 2013;1–16.
18. Mahadevan V. Anatomy of the kidney and ureter. Surg (United Kingdom) [Internet]. 2019;37(7):359–64. Available from: https://doi.org/10.1016/j.mpsur.2019.04.005
19. Samuel L. The anatomy of a kidney [Internet]. Available from: http://www.interactive-biology.com/3254/the-anatomy-of-the-kidney/
20. Moinuddin Z, Dhanda R. Anatomy of the kidney and ureter. Anaesth Intensive Care Med. 2015;16(6):247–52.
21. Vallon V, Mühlbauer B, Osswald H. Adenosine and kidney function. Physiol Rev. 2006;86(3):901–40.
22. Wang X, Garrett MR. Nephron number, hypertension, and CKD: Physiological and genetic insight from humans and animal models. Physiol Genomics. 2017;49(3):180–92.
23. Jörres A, Ronco C, Kellum JA. Managment of acute kidney problems. Berlin, Heidelberg : Springer Berlin Heidelberg : Imprint Springer. 2010.
24. Mital D, Hammes E. Indications for renal transplantation. In: Saclarides, TJ, Myers JA, Millikan KW; Common surgical diseases: An algorithmic approach to problem solving, 3rd ed New York: Springer. 2015. p. 239–42.
25. Weir M, Lerma E. Kidney transplantation. New York, USA: Springer. 2014.
26. Davis CL. Controversies in combined liver-kidney transplantation: indications and outcomes. Transplant Rev. 2008;22(1):82–8.
27. Mekahli D, van Stralen KJ, Bonthuis M, Jager KJ, Balat A, Benetti E, et al. Kidney Versus Combined Kidney and Liver Transplantation in Young People With Autosomal Recessive Polycystic Kidney Disease: Data From the European Society for Pediatric Nephrology/European Renal Association−European Dialysis and Transplant (ESPN/ERA-EDTA). Am J Kidney Dis. 2016;68(5):782–8.
28. Ceulemans LJ, Temmerman F, Jochmans I, Meurisse N, Gilbo N, Monbaliu D, et al. Combined liver and kidney transplantation: listing criteria and results. Transpl Int. 2013;26(2):32.
29. Eurotransplant. Eurotransplant history and time line [Internet]. Available from: https://www.eurotransplant.org/about-eurotransplant/history-and-timelin…
30. Monbaliu D, Loremans P, Ledoux D. Zakboek Orgaan- en weefseldonatie.
31. De Rosner M, Van Rosmalen M, De Boer J, Boogert L, Blok J, Verweij A, et al. Chapter 5 - ET Liver Allocation System (ELAS). In: Eurotransplant Manual. 2019.
32. Desschans B, Van Gelder F, Van Hees D, De Rocy J, Monbaliu D, Aerts R, et al. Evolution in allocation rules for renal, hepatic, pancreatic and intestinal grafts. Acta Chir Belg. 2008;108(1):31–4.
33. De Boer J, Tieken CM. Chapter 4 - Kidney ( ETKAS and ESP ). In: Eurotransplant Manual. 2020. p. 1–32.
34. Jochmans I, Monbaliu D, Ceulemans LJ, Pirenne J, Fronek J. Simultaneous liver kidney transplantation and (bilateral) nephrectomy through a midline is feasible and safe in polycystic disease. PLoS One. 2017;12(3):1–11.
35. Clatworthy M, Watson C, Allison M, Dark J. Transplantation at a glance. 1st ed. Wiley - Blackwell, Ltd; 2012.
36. Farkas S, Hackl C, Schlitt HJ ürge. Overview of the indications and contraindications for liver transplantation. Cold Spring Harb Perspect Med. 2014;4(5):1–14.
37. Lee LY, Foley DP. Technical Aspects of Orthotopic Liver Transplantation for Hepatocellular Carcinoma. Surg Clin North Am [Internet]. 2016;96(2):269–81. Available from: http://dx.doi.org/10.1016/j.suc.2015.11.004
38. Ekser B, Mangus RS, Fridell W, Kubal CA, Nagai S, Kinsella SB, et al. A Novel Approach in Combined Liver and Kidney Transplantation with Long-term Outcomes. Ann Surg. 2017;265(5):1000–8.
39. Hirschfield GM, Gibbs P, Griffiths WJH. Adult liver transplantation: What non-specialists need to know. BMJ. 2009;338(7706):1321–7.
40. Neves DB, Rusi MB, Diaz LGG, Salvalaggio P. Primary graft dysfunction of the liver: definitions, diagnostic criteria and risk factors. Einstein (Sao Paulo). 2016;14(4):567–72.
41. Olthoff K, Kulik L, Samstein B, Kaminski M, Abecassis M, Emond J, et al. Validation of a Current Definition of Early Allograft Dysfunction in Liver Transplant Recipients and Analysis of Risk Factors. Liver Transplant. 2010;16(8):943–9.
42. Lock JF, Schwabauer E, Martus P, Videv N, Pratschke J, Malinowski M, et al. Early Diagnosis of Primary Nonfunction and Indication for Reoperation After Liver Transplantation. Liver Transplant. 2010;16:172–80.
43. Prez-Saborido B, Pacheco-Snchez D, Barrera-Rebollo A, Asensio-Daz E, Pinto-Fuentes P, Sarmentero-Prieto JC, et al. Incidence, management, and results of vascular complications after liver transplantation. Transplant Proc [Internet]. 2011;43(3):749–50. Available from: http://dx.doi.org/10.1016/j.transproceed.2011.01.104
44. Nemes B, Gaman G, Doros A. Biliary complications after liver transplantation. Expert Rev Gastroenterol Hepatol. 2015;9(4):447–66.
45. Mannon RB. Delayed graft function: The AKI of kidney transplantation. Nephron. 2018;140(2):94–8.
46. Mah TJ, Mallon DH, Brewster O, Saeb-Parsy K, Butler AJ, Bradley JA, et al. Ureteric complications in recipients of kidneys from donation after circulatory death donors. Clin Transplant. 2017;31(4):1–6.
47. Feng S, Goodrich NP, Bragg-Gresham JL, Dykstra DM, Punch JD, DebRoy MA, et al. Characteristics associated with liver graft failure: The concept of a donor risk index. Am J Transplant. 2006;6(4):783–90.
48. Pareja E, Cortes M, Hervas D, Mir J, Valdivieso A, Castell J V, et al. A scoring model for the continuous grading or Early Allograft Dysfunction severity. Liver Transplant. 2015;21:38–46.
49. Dindo D, Demartines N, Clavien PA. Classification of surgical complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg. 2004;240(2):205–13.
50. Herrera-Cabezón FJ, Sánchez-Acedo P, Zazpe-Ripa C, Tarifa-Castilla A, Lera-Tricas JM. Quality standards in 480 pancreatic resections: A prospective observational study. Rev Esp Enfermedades Dig. 2015;107(3):143–51.
51. Gilbo N, Jochmans I, Sainz-Barriga M, Nevens F, Van Der Merwe S, Laleman W, et al. Age Matching of Elderly Liver Grafts with Elderly Recipients Does Not Have a Synergistic Effect on Long-term Outcomes When Both Are Carefully Selected. Transplant Direct. 2019;5(4):1–12.
52. Heylen L, Naesens M, Jochmans I, Monbaliu D, Lerut E, Claes K, et al. The effect of anastomosis time on outcome in recipients of kidneys donated after brain death: A cohort study. Am J Transplant. 2015;15(11):2900–7.
53. Doshi SD, Bittermann T, Schiano TD, Goldberg DS. Waitlisted Candidates with Polycystic Liver Disease Are More Likely to be Transplanted Than Those with Chronic Liver Failure. Transplantation. 2017;101(8):1838–44.
54. Lai JC, Covinsky KE, Dodge JL, Boscardin WJ, Segev DL, Roberts JP, et al. Development of a novel frailty index to predict mortality in patients with end-stage liver disease. Hepatology. 2017;66(2):564–74.
55. Montano-Loza A, Meza-Junco J, Baracos V, Prado C, Ma M.D. M, Meeberg G, et al. Severe muscle depletion predicts postoperative length of stay but is not associated with survival after liver transplantation. Liver Transplant. 2014;20(1):640–8.
56. Al-Shraideh Y, Stratta R, Farney A, Orlando G, Palanisamy A, Reeves-Daniel A, et al. Primary non function after deceased donor kidney transplantation: risk en consequences. Transplantation. 2014;98(1):631.
57. Gilbo N, Fieuws S, Meurisse N, Nevens F, van der Merwe S, Laleman W, et al. Donor hepatectomy and implantation time are associated with early complications after liver transplantation: a single centre retrospective study.
58. Melih K V., Basak B, Mustafa C, Nilgun A. Incidence, Risk Factors, and Outcomes of Delayed Graft Function in Deceased Donor Kidney Transplantation. Transplant Proc [Internet]. 2019;51(4):1096–100. Available from: https://doi.org/10.1016/j.transproceed.2019.02.013
59. Rodríguez-Perálvarez M, Rico-Juri JM, Tsochatzis E, Burra P, De la Mata M, Lerut J. Biopsy-proven acute cellular rejection as an efficacy endpoint of randomized trials in liver transplantation: a systematic review and critical appraisal. Transpl Int. 2016;29(9):961–73.
60. Gilbo N, Jochmans I, Sainz M, Pirenne J, Meurisse N, Monbaliu D. Reducing Non-Anastomotic Biliary Strictures in Donation after Circulatory Death Liver Transplantation: Cold Ischemia Time Matters! Ann Surg. 2017;266(6):e118–9.
61. Kivelä JM, Lempinen M, Holmberg C, Jalanko H, Pakarinen MP, Isoniemi H, et al. Renal function after combined liver-kidney transplantation: A longitudinal study of pediatric and adult patients. Pediatr Transplant. 2019;23(4):1–10.
62. Adam R, Bismuth H, Diamond T, Ducot B, Morino M, Astarcioglu I, et al. Effect of extended cold ischaemia with UW solution on graft function after liver transplantation. Lancet. 1992;340(1):1373–6.
63. Totsuka E, Fung JJ, Hakamada K, Ohashi M, Takahashi K, Nakai M, et al. Synergistic Effect of Cold and Warm Ischemia Time on Postoperative Graft Function and Outcome in Human Liver Transplantation. Elsevier. 2004;10–3.
64. Jay C, Pugh J, Halff G, Abrahamian G, Cigarroa F, Washburn K. Graft quality matters: Survival after simultaneous liver-kidney transplant according to KDPI. Vol. 31, Clinical Transplantation. 2017.
65. OPTN, UNOS. A Guide to Calculating and Interpreting the Kidney Donor Profle Index ( KDPI ). 2019;1–11. Available from: https://optn.transplant.hrsa.gov/media/1512/guide_to_calculating_interp…
66. Clavien PA, Camargo C, Croxfors R, Langer B, Levy G, Greig P. Definition and classification of negative outcomes in solid organ transplantation: Application in liver transplantation. Ann Surg. 1994;220(2):109–20.






