
Op zoek naar de maagsonde
- FrédéricClaerhoudt
Tijdens de coronapandemie kwam de dienst intensieve zorgen vaak in het nieuws. Hierdoor zijn de meeste mensen wel bekend met het beeld van een patiënt op intensieve zorgen. Met behulp van allerlei slangetjes en draden wordt de patiënt door machines zo veel mogelijk ondersteund en strikt opgevolgd. Eén van die slangetjes is de maagsonde, een plastic buisje waardoor voeding en medicatie rechtstreeks in de maag van de patiënt kunnen worden toegediend. Deze sonde wordt routinematig door een verpleegkundige gestoken, maar de positie moet na plaatsing steeds gecontroleerd worden. Men zou immers geen voeding willen toedienen wanneer de sonde in de luchtwegen zit en niet in de maag terechtgekomen is. Dit wordt gedaan door middel van (schadelijke) RX-stralen. Frédéric Claerhoudt en Emma Coene, twee studenten geneeskunde aan de Universiteit Gent, onderzochten in volle coronapandemie op de dienst intensieve zorgen of ze deze sonde ook konden lokaliseren met echografie.
Intensieve zorgen
Patiënten op intensieve zorgen zijn meestal niet in staat om zich zelfstandig voldoende te voeden. Daarom wordt de voeding vaak toegediend door hulpverleners. De twee meest voorkomende manieren zijn enerzijds de natuurlijke weg die via een buisje door de neus, langs de keel, in de slokdarm naar de maag loopt of anderzijds via een infuus rechtstreeks in de bloedbaan. Het eerste wordt in de praktijk het meest gebruikt aangezien het goedkoper is en beter voor het maagdarmstelsel. Dit buisje wordt een maagsonde of nasogastrische sonde genoemd.
Maagsonde
De maagsonde wordt vaak geplaatst door een verpleegkundige, zonder dat deze kan zien waar de sonde in het lichaam terecht komt. In 34-58% van de pogingen is de sonde bij de eerste poging juist geplaatst. Deze kan echter ook in de luchtwegen terecht komen (2-3%) (afbeelding 1). Omdat patiënten op intensieve zorgen vaak niet kunnen meewerken of hun ongemak uiten, kan dit onopgemerkt blijven. Indien dan voeding in de longen gegeven wordt, zou 14% van de patiënten overlijden. Dit moet dus ten allen tijde voorkomen worden. Het kan eveneens dat de maagsonde niet diep genoeg geplaatst is en dat ze dus eindigt in de slokdarm. Hierdoor kan voeding terugvloeien en ook in de luchtwegen terecht komen. Daarom is nauwkeurige controle van de plaats van de maagsonde absoluut nodig.
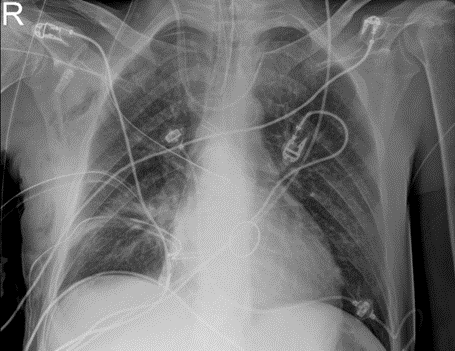
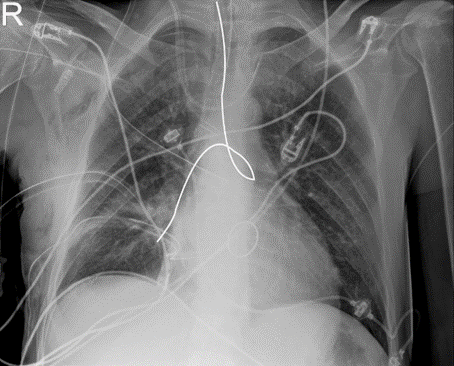 Afbeelding 1: RX bij patiënt met maagsonde die zich in de longen bevindt. Bovenste afbeelding: de originele RX-foto; onderste afbeelding: het verloop van de maagsonde wordt aangegeven door een witte lijn.
Afbeelding 1: RX bij patiënt met maagsonde die zich in de longen bevindt. Bovenste afbeelding: de originele RX-foto; onderste afbeelding: het verloop van de maagsonde wordt aangegeven door een witte lijn.
RX versus echografie
Op een röntgenfoto van de borstkas kan je het verloop van de maagsonde goed zien. Het nemen van die foto kan echter lang op zich laten wachten en daarna moeten de resultaten ook geïnterpreteerd worden. Dit kan zorgen voor vertraging van het toedienen van voeding en medicatie. Daarnaast zijn RX-stralen schadelijk en kunnen hoge dosissen de kans op kanker licht verhogen.
Echografie maakt gebruikt van geluidsgolven om zo een doorsnede van het lichaam te tonen. De maag kan je bekijken door de echoprobe onder de ribbenboog links te plaatsen, de slokdarm kan je visualiseren in de hals. Echografie is goedkoper en gebruikt dus geen schadelijke stralen. Het is ook sneller omdat de arts op intensieve zorgen het toestel ter beschikking heeft en zelf kan gebruiken.
Op het echotoestel is ook een dopplerfunctie aanwezig, die beweging kan detecteren. Als er een mengsel van water en lucht in de sonde wordt gespoten, ziet men als het ware een soort vuurwerk van rood en blauw. Hiermee kan je aantonen dat de sonde weldegelijk in de maag zit.
Werkwijze
Er werd een experimenteel onderzoek met 43 patiënten uitgevoerd. Bij iedere patiënt werd binnen de 30 minuten na plaatsing van de maagsonde een echo van de maag gedaan door de onderzoekers. Iedere patiënt kreeg nog steeds een RX-foto ter controle. Bij de meeste patiënten werd ook een echo van de hals en een dopplerbeeld van de maag bekomen.
Alle data werden hierna statistisch verwerkt waarbij de resultaten van het echo-onderzoek vergeleken werden met de resultaten van de radiografische foto’s.
Resultaten
Het onderzoek toonde aan dat echografie een nuttig onderzoek kan zijn bij patiënten op de dienst intensieve zorgen om de correcte positionering van maagsondes te bevestigen. Bij alle patiënten waarbij het echotoestel aangaf dat de sonde zich in de maag bevond, werd dit bevestigd door de controle radiografische foto’s nadien. Bij 8 patiënten kon het toestel geen sonde visualiseren in de maag. RX-foto's toonden aan dat de sonde bij 7 van deze 8 patiënten toch juist zat. Bij 1 patiënt was de sonde inderdaad verkeerd gestoken en bevond deze zich in de longen.
Protocol
Op basis van de resultaten die hierboven summier beschreven staan, werd een praktisch protocol opgesteld (figuur 1). Er wordt voorgesteld om de sonde eerst op echografische wijze te proberen visualiseren. Indien een echo van de maag de sonde niet kan aantonen, wordt voorgesteld deze te proberen vinden ter hoogte van de hals om te zien of deze zich in de slokdarm bevindt. Indien dit het geval is, kan het immers zijn dat de sonde nog verder opgeschoven moet worden en dat deze dan wel zichtbaar wordt op echo van de maag. Indien een sonde gezien kan worden in de maag, kan een dopplerbeeld gemaakt worden door het inspuiten van een mengsel van water en lucht als extra bevestiging dat de sonde inderdaad op de gevonden plek zit. Indien de correcte positie niet door middel van bovenstaande technieken kan bevestigd worden, dient men toch een RX-foto te nemen. Op deze wijze zou een beduidend deel van de radiografische foto’s vermeden kunnen worden.
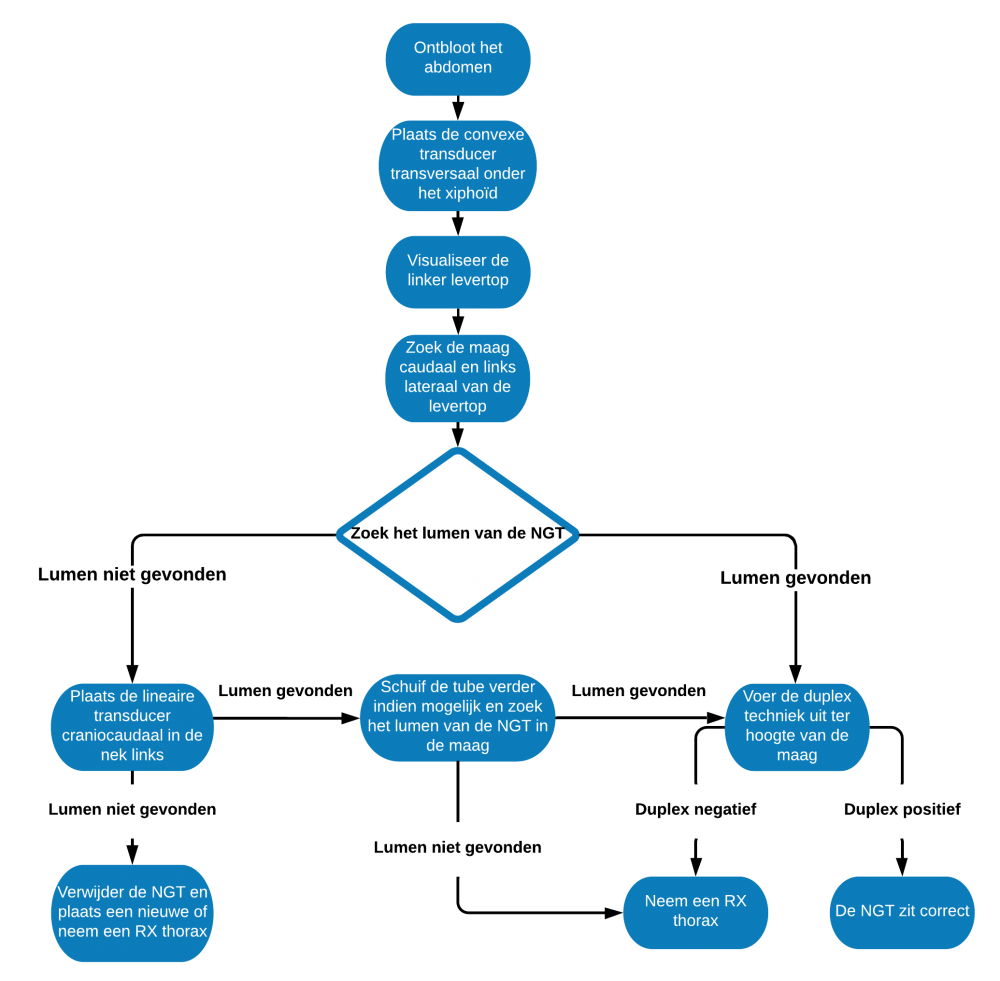
Figuur 1: protocol voor de echografische evaluatie van de correcte positie van een maagsonde.
Conclusie
De studie bevestigt dat echografie bij een geselecteerd aantal patiënten de maagsonde juist kan lokaliseren. Het kan echter niet bij elke patiënt met zekerheid bevestigen dat de maagsonde juist geplaatst is, waardoor echografie niet als alternatief voor RX beschouwd moet worden, maar wel als aanvulling.
Bibliografie
1. Adhikari NK, Fowler RA, Bhagwanjee S, Rubenfeld GD. Critical care and the global burden of critical illness in adults. The Lancet. 2010;376(9749):1339-46.
2.Cho S-H, Hwang JH, Kim J. Nurse staffing and patient mortality in intensive care units. Nurs Res. 2008;57(5):322-30.
3. Colpan A, Akinci E, Erbay A, Balaban N, Bodur H. Evaluation of risk factors for mortality in intensive care units: a prospective study from a referral hospital in Turkey. American journal of infection control. 2005;33(1):42-7.
4. Sciensano. COVID-19 – EPIDEMIOLOGISCH BULLETIN VAN 1 MEI 2021. Sciensanobe2021.
5. Ghahremani GG, Gould RJ. Nasoenteric feeding tubes. Digestive diseases and sciences. 1986;31(6):574-85.
6. Scott R, Bowling TE. Enteral tube feeding in adults. J R Coll Physicians Edinb. 2015;45(1):49- 54.
7. Haslam D, Fang J. Enteral access for nutrition in the intensive care unit. Curr Opin Clin Nutr Metab Care. 2006;9(2):155-9.
8. Koekkoek KW, van Zanten AR. Nutrition in the critically ill patient. Curr Opin Anaesthesiol. 2017;30(2):178-85.
9. Huang HH, Chang SJ, Hsu CW, Chang TM, Kang SP, Liu MY. Severity of illness influences the efficacy of enteral feeding route on clinical outcomes in patients with critical illness. J Acad Nutr Diet. 2012;112(8):1138-46.
10. Luo Y, Qian Y. Effect of combined parenteral and enteral nutrition for patients with a critical illness: A meta-analysis of randomized controlled trials. Medicine (Baltimore). 2020;99(3):e18778.
11. Heyland D. Nutritional support in the critically ill patient: a critical review of the evidence. Critical care clinics. 1998;14(3):423-40.
12. Moore FA, Feliciano DV, Andrassy RJ, McArdle AH, Booth F, Morgenstein-Wagner TB, et al. Early enteral feeding, compared with parenteral, reduces postoperative septic complications. The results of a meta-analysis. Annals of surgery. 1992;216(2):172.
13. Singer P, Berger MM, Van den Berghe G, Biolo G, Calder P, Forbes A, et al. ESPEN guidelines on parenteral nutrition: intensive care. Clinical nutrition. 2009;28(4):387-400.
14. Braunschweig CL, Levy P, Sheean PM, Wang X. Enteral compared with parenteral nutrition: a meta-analysis. The American journal of clinical nutrition. 2001;74(4):534-42.
15. Moore FA, Weisbrodt NW. Gut dysfunction and intolerance to enteral nutrition in critically ill patients. Nestle Nutr Workshop Ser Clin Perform Programme. 2003;8:149-65; discussion 65-70.
16. MacLaren R. Intolerance to intragastric enteral nutrition in critically ill patients: complications and management. Pharmacotherapy. 2000;20(12):1486-98.
17. Gubler C, Bauerfeind P, Vavricka SR, Mullhaupt B, Fried M, Wildi SM. Bedside sonographic control for positioning enteral feeding tubes: a controlled study in intensive care unit patients. Endoscopy. 2006;38(12):1256-60.
18. Itkin M, DeLegge MH, Fang JC, McClave SA, Kundu S, d'Othee BJ, et al. Multidisciplinary practical guidelines for gastrointestinal access for enteral nutrition and decompression from the Society of Interventional Radiology and American Gastroenterological Association (AGA) Institute, with endorsement by Canadian Interventional Radiological Association (CIRA) and Cardiovascular and Interventional Radiological Society of Europe (CIRSE). Gastroenterology. 2011;141(2):742-65.
19. Kreymann K, Berger M, Deutz Ne, Hiesmayr M, Jolliet P, Kazandjiev G, et al. ESPEN guidelines on enteral nutrition: intensive care. Clinical nutrition. 2006;25(2):210-23.
20. Ichimaru S. Methods of Enteral Nutrition Administration in Critically Ill Patients: Continuous, Cyclic, Intermittent, and Bolus Feeding. Nutr Clin Pract. 2018;33(6):790-5.
21. Michel KE. Preventing and managing complications of enteral nutritional support. Clin Tech Small Anim Pract. 2004;19(1):49-53.
22. Crooks NH, Snaith C, Webster D, Gao F, Hawkey P. Clinical review: Probiotics in critical care. Critical Care. 2012;16(6):1-12.
23. Besselink MG, van Santvoort HC, Buskens E, Boermeester MA, van Goor H, Timmerman HM, et al. Probiotic prophylaxis in predicted severe acute pancreatitis: a randomised, double-blind, placebo-controlled trial. The Lancet. 2008;371(9613):651-9.
24. Luft VC, Beghetto MG, de Mello ED, Polanczyk CA. Role of enteral nutrition in the incidence of diarrhea among hospitalized adult patients. Nutrition. 2008;24(6):528-35.
25. de Brito-Ashurst I, Preiser JC. Diarrhea in Critically Ill Patients: The Role of Enteral Feeding. JPEN J Parenter Enteral Nutr. 2016;40(7):913-23.
26. Baskin WN. Acute complications associated with bedside placement of feeding tubes. Nutr Clin Pract. 2006;21(1):40-55.
27. Edes TE, Walk BE, Austin JL. Diarrhea in tube-fed patients: feeding formula not necessarily the cause. Am J Med. 1990;88(2):91-3.
28. Marvin RG, McKinley BA, McQuiggan M, Cocanour CS, Moore FA. Nonocclusive bowel necrosis occurring in critically ill trauma patients receiving enteral nutrition manifests no reliable clinical signs for early detection. Am J Surg. 2000;179(1):7-12.
29. Lord LM. Enteral Access Devices: Types, Function, Care, and Challenges. Nutr Clin Pract. 2018;33(1):16-38.
30. McGinnis CM, Worthington P, Lord LM. Nasogastric versus feeding tubes in critically ill patients. Critical care nurse. 2010;30(6):80-2.
31. Gentilello LM, Cortes V, Castro M, Byers PM. Enteral nutrition with simultaneous gastric decompression in critically ill patients. Critical care medicine. 1993;21(3):392-5.
32. Pearce C, Duncan H. Enteral feeding. Nasogastric, nasojejunal, percutaneous endoscopic gastrostomy, or jejunostomy: its indications and limitations. Postgraduate Medical Journal. 2002;78(918):198-204.
33. Brody H, Hermer LD, Scott LD, Grumbles LL, Kutac JE, McCammon SD. Artificial nutrition and hydration: the evolution of ethics, evidence, and policy. J Gen Intern Med. 2011;26(9):1053-8.
34. Taylor S, Allan K, McWilliam H, Manara A, Brown J, Toher D, et al. Confirming nasogastric tube position with electromagnetic tracking versus pH or X-ray and tube radio-opacity. Br J Nurs. 2014;23(7):352, 4-8.
35. Sanaie S, Mahmoodpoor A, Najafi M. Nasogastric tube insertion in anaesthetized patients: a comprehensive review. Anaesthesiol Intensive Ther. 2017;49(1):57-65.
36. Metheny NA, Krieger MM, Healey F, Meert KL. A review of guidelines to distinguish between gastric and pulmonary placement of nasogastric tubes. Heart Lung. 2019;48(3):226-35.
37. Appukutty J, Shroff PP. Nasogastric tube insertion using different techniques in anesthetized patients: a prospective, randomized study. Anesthesia and analgesia. 2009;109(3):832-5.
38. Mahajan R, Gupta R, Sharma A. Role of neck flexion in facilitating nasogastric tube insertion. Anesthesiology. 2005;103(2):446-7.
39. Bong CL, Macachor JD, Hwang NC. Insertion of the nasogastric tube made easy. Anesthesiology. 2004;101(1):266.
40. Chun DH, Kim NY, Shin YS, Kim SH. A randomized, clinical trial of frozen versus standard nasogastric tube placement. World journal of surgery. 2009;33(9):1789-92.
41. de Aguilar‐Nascimento JE, Kudsk KA. Clinical costs of feeding tube placement. Journal of Parenteral and Enteral Nutrition. 2007;31(4):269-73.
42. Sparks DA, Chase DM, Coughlin LM, Perry E. Pulmonary complications of 9931 narrow-bore nasoenteric tubes during blind placement: a critical review. JPEN Journal of parenteral and enteral nutrition. 2011;35(5):625-9.
43. Sorokin R, Gottlieb JE. Enhancing patient safety during feeding‐tube insertion: a review of more than 2000 insertions. Journal of Parenteral and Enteral Nutrition. 2006;30(5):440-5.
44. Marderstein EL, Simmons RL, Ochoa JB. Patient safety: effect of institutional protocols on adverse events related to feeding tube placement in the critically ill. J Am Coll Surg. 2004;199(1):39- 47; discussion -50.
45. Agency NPS. Patient Safety Alert NPSA/2011/PSA002: Reducing the harm caused by misplaced nasogastric feeding tubes in adults, children and infants. National Patient Safety Agency London; 2011.
46. Taylor SJ, Allan K, McWilliam H, Toher D. Nasogastric tube depth: the 'NEX' guideline is incorrect. Br J Nurs. 2014;23(12):641-4.
47. Ratzlaff HC, Heaslip JE, Rothwell ES. Factors affecting nasogastric tube insertion. Critical care medicine. 1984;12(1):52-3.
48. Najafi M, Golzari SE. SORT maneuver for nasogastric tube insertion. Anaesthesia. 2016;71(3):351.
49. Sanaie S, Mirzalou N, Shadvar K, Golzari SEJ, Soleimanpour H, Shamekh A, et al. A comparison of nasogastric tube insertion by SORT maneuver (sniffing position, NGT orientation, contralateral rotation, and twisting movement) versus neck flexion lateral pressure in critically ill patients admitted to ICU: a prospective randomized clinical trial. Ann Intensive Care. 2020;10(1):79.
50. Shastri YM, Shirodkar M, Mallath MK. Endoscopic feeding tube placement in patients with cancer: a prospective clinical audit of 2055 procedures in 1866 patients. Aliment Pharmacol Ther. 2008;27(8):649-58.
51. Powers J, Luebbehusen M, Aguirre L, Cluff J, David MA, Holly V, et al. Improved Safety and Efficacy of Small-Bore Feeding Tube Confirmation Using an Electromagnetic Placement Device. Nutr Clin Pract. 2018;33(2):268-73.
52. Bercik P, Schlageter V, Mauro M, Rawlinson J, Kucera P, Armstrong D. Noninvasive verification of nasogastric tube placement using a magnet-tracking system: a pilot study in healthy subjects. JPEN Journal of parenteral and enteral nutrition. 2005;29(4):305-10.
53. Gao X, Zhang L, Zhao J, Tian F, Sun H, Wang P, et al. Bedside electromagnetic-guided placement of nasoenteral feeding tubes among critically Ill patients: A single-centre randomized controlled trial. J Crit Care. 2018;48:216-21.
54. Gok F, Kilicaslan A, Yosunkaya A. Ultrasound‐guided nasogastric feeding tube placement in critical care patients. Nutrition in Clinical Practice. 2015;30(2):257-60.
55. Mizzi A, Cozzi S, Beretta L, Greco M, Braga M. Real-time image-guided nasogastric feeding tube placement: A case series using Kangaroo with IRIS Technology in an ICU. Nutrition. 2017;37:48- 52.
56. Pillai JB, Vegas A, Brister S. Thoracic complications of nasogastric tube: review of safe practice. Interact Cardiovasc Thorac Surg. 2005;4(5):429-33.
57. George DL, Falk PS, Umberto Meduri G, Leeper KV, Jr., Wunderink RG, Steere EL, et al. Nosocomial sinusitis in patients in the medical intensive care unit: a prospective epidemiological study. Clin Infect Dis. 1998;27(3):463-70.
58. Patrick PG, Marulendra S, Kirby DF, DeLegge MH. Endoscopic nasogastric-jejunal feeding tube placement in critically ill patients. Gastrointestinal endoscopy. 1997;45(1):72-6.
59. Powell KS, Marcuard SP, Farrior ES, Gallagher ML. Aspirating gastric residuals causes occlusion of small-bore feeding tubes. JPEN Journal of parenteral and enteral nutrition. 1993;17(3):243-6.
60. Agarwal A, Gaur A, Sahu D, Singh PK, Pandey CK. Nasogastric tube knotting over the epiglottis: a cause of respiratory distress. Anesth Analg. 2002;94(6):1659-60, table of contents.
61. Monib S, ElKorety M, Jibrin U, Dhungana D, Thomson S. Knotted nasogastric tube: a rare, overlooked yet preventable complication. J Surg Case Rep. 2019;2019(10):rjz290.
62. Chavda V, Alhammali T, Farrant J, Naidu L, El-Rabaa S. Nasogastric tube knotting: a rare and potentially overlooked complication among healthcare professionals. BMJ Case Rep. 2017;2017.
63. Santhanam V, Margarson M. Removal of self-knotted nasogastric tube: technical note. Int J Oral Maxillofac Surg. 2008;37(4):384-5.
64. Tai CM, Wang HP, Lee CT, Chang CY, Wang WL, Tseng CH, et al. Esophageal obstruction by a tangled nasogastric tube. Gastrointestinal endoscopy. 2010;72(5):1057-8.
65. Wright S, Warusavitarne J, Shaikh I. Safe removal of knotted nasogastric tubes. Nursing Times. 2014;110(43):16-7.
66. Williams A, Liddle D, Singh AK. A knotted nasogastric tube. Anesth Essays Res. 2011;5(1):109- 10.
67. Ravind R, Prameela CG, Gurram BC, Dinesh M. Naughty knot: a case of nasogastric tube knotting. BMJ case reports. 2015;2015.
68. Metheny NA, Meert KL, Clouse RE. Complications related to feeding tube placement. Curr Opin Gastroenterol. 2007;23(2):178-82.
69. L Miller S. Capnometry vs pH testing in nasogastric tube placement. Gastrointestinal Nursing. 2011;9(2):30-3.
70. Paparoupa M, Yan Y, Möller M, Schuppert F. Nasogastric tube ending in the right pleura of an intubated patient. Intensive Care Med. 2019;45(4):523-4.
71. Sankar V, Shakeel M, Keh S, Ah-See KW. A case of a 'lost' nasogastric tube. J Laryngol Otol. 2012;126(12):1296-8.
72. Koo S. Nasogastric tube check, easy or not? BMJ Case Rep. 2016;2016.
73. Takwoingi YM. Inadvertent insertion of a nasogastric tube into both main bronchi of an awake patient: a case report. Cases J. 2009;2:6914.
74. Fonseca VR, Domingos G, Alves P, Ribeiro R. Placement of nasogastric tube complicated by hydropneumothorax. Intensive Care Med. 2015;41(11):1969-70.
75. Johnstone JC, Leung JS, Friedman JN. Nasogastric tube misadventures. Clin Pediatr (Phila). 2011;50(10):983-6.
76. Mohiuddin SA, Al Kaabi S, Butt T, Yakoob R, Khanna M. Down the wrong road - a case report of inadvertent nasogastric tube insertion leading to lung laceration and important pearls to avoid complications. Qatar Med J. 2016;2016(2):12.
77. Improvement N. Never Events list 2018. 2018.
78. Metheny NA, Clouse RE, Chang YH, Stewart BJ, Oliver DA, Kollef MH. Tracheobronchial aspiration of gastric contents in critically ill tube-fed patients: frequency, outcomes, and risk factors. Crit Care Med. 2006;34(4):1007-15.
79. Seguin P, Le Bouquin V, Aguillon D, Maurice A, Laviolle B, Mallédant Y. [Testing nasogastric tube placement: evaluation of three different methods in intensive care unit]. Ann Fr Anesth Reanim. 2005;24(6):594-9.
80. Isik A, Firat D, Peker K, Sayar I, Idiz O, Soytürk M. A case report of esophageal perforation: Complication of nasogastric tube placement. Am J Case Rep. 2014;15:168-71.
81. Ryom P, Ravn JB, Penninga L, Schmidt S, Iversen MG, Skov-Olsen P, et al. Aetiology, treatment and mortality after oesophageal perforation in Denmark. Dan Med Bull. 2011;58(5):A4267.
82. Vidarsdottir H, Blondal S, Alfredsson H, Geirsson A, Gudbjartsson T. Oesophageal perforations in Iceland: a whole population study on incidence, aetiology and surgical outcome. Thorac Cardiovasc Surg. 2010;58(8):476-80.
83. Mileder LP, Müller M, Reiterer F, Pilhatsch A, Gürtl-Lackner B, Urlesberger B, et al. Esophageal Perforation with Unilateral Fluidothorax Caused by Nasogastric Tube. Case Rep Pediatr. 2016;2016:4103734.
84. Tawfic QA, Bhakta P, Date RR, Sharma PK. Esophageal bezoar formation due to solidification of enteral feed administered through a malpositioned nasogastric tube: case report and review of the literature. Acta Anaesthesiol Taiwan. 2012;50(4):188-90.
85. Janicki A, Van Ginkel C, Cohn J. Gastric Perforation Following Nasogastric Intubation in an Elderly Male. R I Med J (2013). 2015;98(9):45-6.
86. Allen F, Riopelle J, Sinha A. Case report: intracranial placement of a nasotracheal tube in a patient with Goldenhar syndrome associated with cribriform plate agenesis. Anesth Analg. 2011;112(1):198-200.
87. Ferreras J, Junquera LM, García-Consuegra L. Intracranial placement of a nasogastric tube after severe craniofacial trauma. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2000;90(5):564- 6.
88. Hanna AS, Grindle CR, Patel AA, Rosen MR, Evans JJ. Inadvertent insertion of nasogastric tube into the brain stem and spinal cord after endoscopic skull base surgery. Am J Otolaryngol. 2012;33(1):178-80.
89. Psarras K, Lalountas MA, Symeonidis NG, Baltatzis M, Pavlidis ET, Ballas K, et al. Inadvertent insertion of a nasogastric tube into the brain: case report and review of the literature. Clin Imaging. 2012;36(5):587-90.
90. Rahimi-Movaghar V, Boroojeny SB, Moghtaderi A, Keshmirian B. Intracranial placement of a nasogastric tube. A lesson to be re-learnt? Acta Neurochir (Wien). 2005;147(5):573-4; discussion 4.
91. Zhang X, Ji T, Chen L, Yang J, Huang G. Nasogastric Tube Feeding into Brain After Endoscopic Endonasal Transsphenoidal Surgery. World Neurosurg. 2019;132:4-6.
92. Adler JS, Graeb DA, Nugent RA. Inadvertent intracranial placement of a nasogastric tube in a patient with severe head trauma. Cmaj. 1992;147(5):668-9.
93. Viteri G, Larrache J, Díaz ML, Alcalde JM, Lopez-Olaondo L, Bilbao JI. Nasogastric tube found in the right atrium. J Vasc Interv Radiol. 2012;23(5):721-2.
94. Longo MA. Best evidence: nasogastric tube placement verification. J Pediatr Nurs. 2011;26(4):373-6.
95. Durai R, Venkatraman R, Ng P. Nasogastric tubes. 1: Insertion technique and confirming the correct position. Nursing times. 2009;105(16):12-3.
96. Fan EMP, Tan SB, Ang SY. Nasogastric tube placement confirmation: Where we are and where we should be heading. Proceedings of Singapore Healthcare. 2017;26(3):189-95.
97. Taylor SJ. Confirming nasogastric feeding tube position versus the need to feed. Intensive Crit Care Nurs. 2013;29(2):59-69.
98. Chenaitia H, Brun P-M, Querellou E, Leyral J, Bessereau J, Aimé C, et al. Ultrasound to confirm gastric tube placement in prehospital management. Resuscitation. 2012;83(4):447-51.
99. Irving SY, Lyman B, Northington L, Bartlett JA, Kemper C. Nasogastric tube placement and verification in children: review of the current literature. Nutr Clin Pract. 2014;29(3):267-76.
100. Irving SY, Rempel G, Lyman B, Sevilla WMA, Northington L, Guenter P. Pediatric Nasogastric Tube Placement and Verification: Best Practice Recommendations From the NOVEL Project. Nutr Clin Pract. 2018;33(6):921-7.
101. Atalay YO, Aydin R, Ertugrul O, Gul SB, Polat AV, Paksu MS. Does Bedside Sonography Effectively Identify Nasogastric Tube Placements in Pediatric Critical Care Patients? Nutr Clin Pract. 2016;31(6):805-9.
102. Dağlı R, Bayır H, Dadalı Y, Tokmak TT, Erbesler ZA. Role of Ultrasonography in Detecting the Localisation of the Nasoenteric Tube. Turk J Anaesthesiol Reanim. 2017;45(2):103-7.
103. Srinivasan S, Cornell TT. Bedside ultrasound in pediatric critical care: a review. Pediatric Critical Care Medicine. 2011;12(6):667.
104. Vigneau C, Baudel J-L, Guidet B, Offenstadt G, Maury E. Sonography as an alternative to radiography for nasogastric feeding tube location. Intensive care medicine. 2005;31(11):1570-2.
105. Kim HM, So BH, Jeong WJ, Choi SM, Park KN. The effectiveness of ultrasonography in verifying the placement of a nasogastric tube in patients with low consciousness at an emergency center. Scand J Trauma Resusc Emerg Med. 2012;20:38.
106. Lin T, Gifford W, Lan Y, Qin X, Liu X, Wang J, et al. Diagnostic accuracy of ultrasonography for detecting nasogastric tube (NGT) placement in adults: A systematic review and meta analysis. Int J Nurs Stud. 2017;71:80-8.
107. Claiborne MK, Gross T, McGreevy J, Riemann M, Temkit M, Augenstein J. Point-of-Care Ultrasound for Confirmation of Nasogastric and Orogastric Tube Placement in Pediatric Patients. Pediatr Emerg Care. 2020.
108. Metheny NA. Insufficient evidence to support ultrasonography as a method to rule out an improperly positioned nasogastric tube. Evid Based Nurs. 2018;21(3):79.
109. Yıldırım Ç, Coşkun S, Gökhan Ş, Pamukçu Günaydın G, Özhasenekler A, Özkula U. Verifying the Placement of Nasogastric Tubes at an Emergency Center: Comparison of Ultrasound with Chest Radiograph. Emerg Med Int. 2018;2018:2370426.
110. Zatelli M, Vezzali N. 4-Point ultrasonography to confirm the correct position of the nasogastric tube in 114 critically ill patients. Journal of ultrasound. 2017;20(1):53-8.
111. Brun P-M, Chenaitia H, Lablanche C, Pradel A-L, Deniel C, Bessereau J, et al. 2-point ultrasonography to confirm correct position of the gastric tube in prehospital setting. Military medicine. 2014;179(9):959-63.
112. Neumann MJ, Meyer CT, Dutton JL, Smith R. Hold that x-ray: aspirate pH and auscultation prove enteral tube placement. J Clin Gastroenterol. 1995;20(4):293-5.
113. Boeykens K, Steeman E, Duysburgh I. Reliability of pH measurement and the auscultatory method to confirm the position of a nasogastric tube. Int J Nurs Stud. 2014;51(11):1427-33.
114. Simons SR, Abdallah LM. Bedside assessment of enteral tube placement: aligning practice with evidence. Am J Nurs. 2012;112(2):40-6; quiz 8, 7.
115. Metheny NA, Stewart BJ, Smith L, Yan H, Diebold M, Clouse RE. pH and concentration of bilirubin in feeding tube aspirates as predictors of tube placement. Nurs Res. 1999;48(4):189-97.
116. Bourgault AM, Halm MA. Feeding tube placement in adults: safe verification method for blindly inserted tubes. American Journal of Critical Care. 2009;18(1):73-6.
117. Rowat AM, Graham C, Dennis M. Study to determine the likely accuracy of pH testing to confirm nasogastric tube placement. BMJ Open Gastroenterol. 2018;5(1):e000211.
118. Muslu B, Demircioglu RI, Gözdemir M, Usta B. Comparison of neck ultrasonography with a pH meter to confirm correct position of nasogastric tube. Clin Invest Med. 2016;39(6):27520.
119. Anderson O, Carr R, Harbinson M, Hanna GB. Development and validation of a lipase nasogastric tube position test. BMJ Open Gastroenterol. 2016;3(1):e000064.
120. Taylor SJ, Clemente R. Confirmation of nasogastric tube position by pH testing. J Hum Nutr Diet. 2005;18(5):371-5.
121. Gilbertson HR, Rogers EJ, Ukoumunne OC. Determination of a practical pH cutoff level for reliable confirmation of nasogastric tube placement. JPEN Journal of parenteral and enteral nutrition. 2011;35(4):540-4.
122. Rowat AM, Graham C, Dennis M. Diagnostic accuracy of a pH stick, modified to detect gastric lipase, to confirm the correct placement of nasogastric tubes. BMJ Open Gastroenterol. 2018;5(1):e000218.
123. Fordtran JS, Walsh JH. Gastric acid secretion rate and buffer content of the stomach after eating. Results in normal subjects and in patients with duodenal ulcer. J Clin Invest. 1973;52(3):645- 57.
124. Lanas A, Artal A, Blás JM, Arroyo MT, Lopez-Zaborras J, Sáinz R. Effect of parenteral omeprazole and ranitidine on gastric pH and the outcome of bleeding peptic ulcer. J Clin Gastroenterol. 1995;21(2):103-6.
125. Metheny NA. Inadvertent intracranial nasogastric tube placement. Am J Nurs. 2002;102(8):25-7.
126. Sahn SA. State of the art. The pleura. Am Rev Respir Dis. 1988;138(1):184-234.
127. Mise K, Capkun V, Jurcev-Savicevic A, Sundov Z, Bradaric A, Mladinov S. The influence of gastroesophageal reflux in the lung: a case-control study. Respirology. 2010;15(5):837-42.
128. Borsci S, Buckle P, Huddy J, Alaestante Z, Ni Z, Hanna GB. Usability study of pH strips for nasogastric tube placement. PloS one. 2017;12(11):e0189013.
129. Fernandez RS, Chau JP, Thompson DR, Griffiths R, Lo HS. Accuracy of biochemical markers for predicting nasogastric tube placement in adults--a systematic review of diagnostic studies. Int J Nurs Stud. 2010;47(8):1037-46.
130. Metheny NA, Smith L, Stewart BJ. Development of a reliable and valid bedside test for bilirubin and its utility for improving prediction of feeding tube location. Nurs Res. 2000;49(6):302-9.
131. Metheny NA, Stewart BJ, Smith L, Yan H, Diebold M, Clouse RE. pH and concentrations of pepsin and trypsin in feeding tube aspirates as predictors of tube placement. JPEN Journal of parenteral and enteral nutrition. 1997;21(5):279-85.
132. Munera-Seeley V, Ochoa JB, Brown N, Bayless A, Correia MI, Bryk J, et al. Use of a colorimetric carbon dioxide sensor for nasoenteric feeding tube placement in critical care patients compared with clinical methods and radiography. Nutr Clin Pract. 2008;23(3):318-21.
133. Chau JP, Lo SH, Thompson DR, Fernandez R, Griffiths R. Use of end-tidal carbon dioxide detection to determine correct placement of nasogastric tube: a meta-analysis. Int J Nurs Stud. 2011;48(4):513-21.
134. Burns SM, Carpenter R, Blevins C, Bragg S, Marshall M, Browne L, et al. Detection of inadvertent airway intubation during gastric tube insertion: Capnography versus a colorimetric carbon dioxide detector. American journal of critical care : an official publication, American Association of Critical-Care Nurses. 2006;15(2):188-95.
135. Mordiffi SZ, Goh ML, Phua J, Chan YH. Confirming nasogastric tube placement: Is the colorimeter as sensitive and specific as X-ray? A diagnostic accuracy study. Int J Nurs Stud. 2016;61:248-57.
136. Bennetzen LV, Håkonsen SJ, Svenningsen H, Larsen P. Diagnostic accuracy of methods used to verify nasogastric tube position in mechanically ventilated adult patients: a systematic review. JBI Database System Rev Implement Rep. 2015;13(1):188-223.
137. Howes DW, Shelley ES, Pickett W. Colorimetric carbon dioxide detector to determine accidental tracheal feeding tube placement. Can J Anaesth. 2005;52(4):428-32.
138. Kindopp AS, Drover JW, Heyland DK. Capnography confirms correct feeding tube placement in intensive care unit patients. Can J Anaesth. 2001;48(7):705-10.
139. Elpern EH, Killeen K, Talla E, Perez G, Gurka D. Capnometry and air insufflation for assessing initial placement of gastric tubes. American journal of critical care : an official publication, American Association of Critical-Care Nurses. 2007;16(6):544-9; quiz 50.
140. Meyer P, Henry M, Maury E, Baudel JL, Guidet B, Offenstadt G. Colorimetric capnography to ensure correct nasogastric tube position. J Crit Care. 2009;24(2):231-5.
141. Boyes RJ, Kruse JA. Nasogastric and nasoenteric intubation. Critical care clinics. 1992;8(4):865-78.
142. Bowers S. Tubes: a nurse's guide to enteral feeding devices. Medsurg Nurs. 1996;5(5):313- 24; quiz 25-6.
143. Welch SK. Certification of staff nurses to insert enteral feeding tubes using a research-based procedure. Nutr Clin Pract. 1996;11(1):21-7.
144. Raff MH, Cho S, Dale R. A technique for positioning nasoenteral feeding tubes. JPEN Journal of parenteral and enteral nutrition. 1987;11(2):210-3.
145. Prasad G, Garg R. The 'bubble technique': an innovative technique for confirming correct nasogastric tube placement. J Clin Anesth. 2011;23(1):84-5.
146. Chang JL, Melnick B, Bedger RC, Bleyaert AL. Inadvertent endobronchial intubation with nasogastric tube. Occurrence after head and neck surgery. Arch Otolaryngol. 1982;108(8):528-9.
147. Metheny N, Dettenmeier P, Hampton K, Wiersema L, Williams P. Detection of inadvertent respiratory placement of small-bore feeding tubes: a report of 10 cases. Heart & lung : the journal of critical care. 1990;19(6):631-8.
148. Agency NPS. Reducing Harm Caused by the Misplacement of Nasogastric Feeding Tubes. NPSA London, UK; 2005.
149. Turgay AS, Khorshid L. Effectiveness of the auscultatory and pH methods in predicting feeding tube placement. J Clin Nurs. 2010;19(11-12):1553-9.
150. Metheny N, Wehrle MA, Wiersema L, Clark J. Testing feeding tube placement. Auscultation vs. pH method. Am J Nurs. 1998;98(5):37-42; quiz -3.
151. Benya R, Langer S, Mobarhan S. Flexible nasogastric feeding tube tip malposition immediately after placement. JPEN Journal of parenteral and enteral nutrition. 1990;14(1):108-9.
152. Hendry PJ, Akyurekli Y, McIntyre R, Quarrington A, Keon WJ. Bronchopleural complications of nasogastric feeding tubes. Critical care medicine. 1986;14(10):892-4.
153. Hand RW, Kempster M, Levy JH, Rogol PR, Spirn P. Inadvertent transbronchial insertion of narrow-bore feeding tubes into the pleural space. Jama. 1984;251(18):2396-7.
154. Dobranowski J, Fitzgerald JM, Baxter F, Woods D. Incorrect positioning of nasogastric feeding tubes and the development of pneumothorax. Can Assoc Radiol J. 1992;43(1):35-9.
155. McWey RE, Curry NS, Schabel SI, Reines HD. Complications of nasoenteric feeding tubes. Am J Surg. 1988;155(2):253-7.
156. Metheny NA, Stewart BJ. Testing feeding tube placement during continuous tube feedings. Appl Nurs Res. 2002;15(4):254-8.
157. Paul V, Shenoy A, Kupfer Y, Tessler S. Pneumothorax occurring after nasogastric tube removal. BMJ Case Rep. 2013;2013.
158. Winterholler M, Erbguth FJ. Accidental pneumothorax from a nasogastric tube in a patient with severe hemineglect: a case report. Arch Phys Med Rehabil. 2002;83(8):1173-4.
159. Bear DE, Champion A, Lei K, Smith J, Beale R, Camporota L, et al. Use of an Electromagnetic Device Compared With Chest X-ray to Confirm Nasogastric Feeding Tube Position in Critical Care. JPEN J Parenter Enteral Nutr. 2016;40(4):581-6.
160. vragen-factuur. Available from: https://www.uzgent.be/nl/patienten/betaling/vragen- factuur/Paginas/default.aspx.
161. Piton G, Parel R, Delabrousse E, Capellier G. Echography for nasogastric tube placement verification. Eur J Clin Nutr. 2017;71(5):669-70.










